
Журнал "Гастроэнтерология" Том 56, №4, 2022
Вернуться к номеру
Обмеження та значення неінвазивного тесту для оцінки хронічного захворювання печінки
Авторы: V. Siva Kesava Reddy, Shubham Nimkar, Mansi Patel, Sourya Acharya
Jawaharlal Nehru Medical College, Datta Meghe Institute of Medical Sciences (Deemed to be University), Sawangi (Meghe), Wardha, Maharashtra, India
Рубрики: Гастроэнтерология
Разделы: Справочник специалиста
Версия для печати
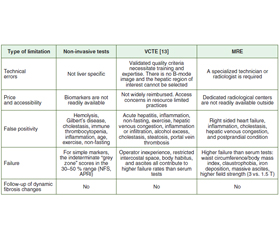
Золотим стандартом для оцінки фіброзу печінки є її біопсія. Однак ця процедура інвазивна і пов’язана з болем, а іноді й зі смертельними наслідками. Точність результатів біопсії печінки ще більше погіршується внаслідок варіабельності результатів в одного та різних дослідників. Використовуються тільки невеликі зразки. Це призводить до змішування двох типів варіабельності, про які говорилося вище. Через ці обмеження були розроблені неінвазивні підходи до скринінгу на фіброз. Різні біохімічні показники сироватки крові або методи візуалізації, що забезпечують фізичне вимірювання жорсткості печінки, дозволяють неінвазивно оцінити фіброз печінки.
The gold standard for assessing liver fibrosis is a liver biopsy. However, the procedure is invasive and is associated with pain and sometimes fatal consequences. The accuracy of liver biopsy results is further harmed by intra- and inter-observer variability. Small samples only. This muddles the two types of observer variability discussed above. Due to these limitations, non-invasive approaches for fibrosis testing have been developed. Various biochemical serum indicators or imaging techniques that provide a physical measure of hepatic stiffness are non-invasive approaches for assessing liver fibrosis.
оцінка жорсткості печінки; транзиторна еластографія; магнітно-резонансна еластографія; ФіброТест; хронічні захворювання печінки; хронічний гепатит В; цироз печінки; індекс співвідношення аспартатамінотрансферази до тромбоцитів
liver stiffness assessment; transient elastography; magnetic resonance elastography; FibroTest; chronic liver disease; chronic hepatitis B; cirrhosis; aspartate aminotransferase-to-platelet ratio index
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Patel K, Sebastiani G. Limitations of non-invasive tests for assessment of liver fibrosis. JHEP Rep. 2020;2(2):100067. doi: 10.1016/j.jhepr.2020.100067.
- Salkic NN, Jovanovic P, Hauser G, Brcic M. FibroTest/Fibrosure for significant liver fibrosis and cirrhosis in chronic hepatitis B: a meta-analysis. Am J Gastroenterol. 2014;109:796-809. doi: 10.1038/ajg.2014.21.
- Kumar M, Sarin SK, Hissar S, Pande C, Sakhuja P, Sharma BC. Virologic and histologic features of chronic hepatitis B virus-infected asymptomatic patients with persistently normal ALT. Gastroenterology. 2008;134:1376-1384. doi: 10.1053/j.gastro.2008.02.075.
- Marcellin P, Gane E, Buti M, Afdhal N, Sievert W, Jacobson IM. Regression of cirrhosis during treatment with tenofovir disoproxil fumarate for chronic hepatitis B: a 5-year open-label follow-up study. Lancet. 2013;381(9865):468-475. doi: 10.1016/S0140-6736(12)61425-1.
- Chang TT, Liaw YF, Wu SS, Schiff E, Han KH, Lai CL. Long-term entecavir therapy results in the reversal of fibrosis/cirrhosis and continued histological improvement in patients with chronic hepatitis B. Hepatology. 2010;52:886-893. doi: 10.1002/hep.23785.
- Lee S, Kim DY. Non-invasive diagnosis of hepatitis B virus-related cirrhosis. World J Gastroenterol. 2014;20(2):445-459. doi: 10.3748/wjg.v20.i2.445.
- Castera L, Foucher J, Bernard PH et al. Pitfalls of liver stiffness measurement: a 5-year prospective study of 13,369 examinations. Hepatology. 2010;51:828-835. doi: 10.1002/hep.23425.
- Wong GL, Wong VW, Chim AM et al. Factors associated with unreliable liver stiffness measurement and its failure with transient elastography in the Chinese population. J Gastroenterol Hepatol. 2011;26:300-305. doi: 10.1111/j.1440-1746.2010.06510.x.
- Boursier J, Zarski JP, de Ledinghen V et al. Determination of reliability criteria for liver stiffness evaluation by transient elastography. Hepatology. 2013;57:1182-1191. doi: 10.1002/hep.25993.
- Das K, Sarkar R, Ahmed SM, Mridha AR, Mukherjee PS, Dhali GK et al. “Normal” liver stiffness measure (LSM) values are higher in both lean and obese individuals: a population-based study from a developing country. Hepatology. 2012;55:584-593. doi: 10.1002/hep.24694.
- Myers RP, Pomier-Layrargues G, Kirsch R, Pollett A, Duarte-Rojo A, Wong D et al. Feasibility and diagnostic performance of the FibroScan XL probe for liver stiffness measurement in overweight and obese patients. Hepatology. 2012;55:199-208. doi: 10.1002/hep.24624.
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO) EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. Diabetologia. 2016;59:1121-1140. doi: 10.1016/j.jhep.2015.11.004.
- Tapper EB, Castera L, Afdhal NH. FibroScan (vibration-controlled transient elastography): where does it stand in the United States practice. Clin Gastroenterol Hepatol. 2014;13:27-36. doi:10.1016/j.cgh.2014.04.039.