Introduction
In December 2019, a series of unknown origin cases of acute respiratory illness occurred in Wuhan, Hubei Province, China. High-throughput sequencing showed that the disease was caused by named “severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2). On February 11, 2020, the World Health Organization officially changed the name of the disease caused by SARS-CoV-2 to coronavirus disease 2019 (COVID-19). Although diffuse alveolar damage and acute respiratory failure were the main features of COVID-19, the involvement of other organs needed to be explored. After lung infection, the virus may enter the blood, accumulate in kidney, and cause damage to resident renal cells. Indeed, COVID-19 RNA was found in the plasma of 15 % of patients by real-time polymerase chain reaction. Of note, it is reported showed that 6.7 % of patients with SARS developed acute kidney injury (AKI, and the mortality of those with AKI was 91.7 %. Thus, understanding how the kidney is affected by SARS-CoV-2 is urgently warranted [1].
A recent prospective cohort study reviewed kidney disease among 701 patients who were treated for COVID-19 in Wuhan, China. Those patients with kidney disease had higher in-hospital mortality; moreover, there was evidence of hematuria in 26.7 % and proteinuria in 43.9 % of patients in their cohort. Although kidney tissue was not examined, the authors postulated potential multifactorial renal injury, including direct cytopathic effects (via viral entry through angiotensin-converting enzyme 2 receptors expressed on tubular epithelium), as well as tubular injury from cytokine storm, shock, and rhabdomyolysis [2]. High comorbidity in this case increases the risk of kidney damage in COVID-19 (chronic kidney disease, heart failure, liver disease, diabetes mellitus, acute kidney damage in the anamnesis, patient age > 65 years) [3].
It is unlikely that SARS-CoV-2 directly causes primary liver injury but the mechanisms by which SARS-CoV-2 affects the liver are not well defined. Postmortem studies report moderate microvascular steatosis with mild lobular and portal activity but no obvious inflammatory cell infiltration or typical liver cell necrosis. Ultrastructural examination from 2 COVID-19 patients identified typical, spike structure coronavirus particles in the cytoplasm of hepatocytes accompanied by massive hepatic apoptosis, some binuclear hepatocytes and scanty CD4+ and CD8+ lymphocytes that were considered indicative of a typical viral infection. A proposed mechanism of direct liver injury is by direct cytotoxicity from viral replication in liver cells [4]. The most significant modifiable risk factors for the poor prognosis from COVID-19 are obesity and metabolic disease. These findings, such as nonalcoholic fatty liver disease (NAFLD), cause the activation of inflammatory pathways. It suggests that NAFLD can play a key role as a risk factor in the severity and prognosis of coronavirus disease 2019 patients [5].
Therefore, research aimed at determining the possible mechanisms of progression in the damage to various organs and systems against the background of COVID-19 infection is an urgent, not thoroughly studied issue in contemporary clinical medicine. The study of the influence of biologically active substances that regulate various physiological processes in the human body, including enhancing antioxidant, immune-regulating systems, is of particular interest. In this connection, it is relevant to consider the effect of neurohormones, such as melatonin (MT) and its precursor — serotonin (ST). Nowadays, it is possible to distinguish 7 families of serotonin receptors, which trigger intracellular processes affecting the excitation of other mediator systems and manifest metabolitotropic effects, i.e., they activate the cascade of intracellular biochemical reactions in the target cells [6]. Melatonin is secreted by the epiphysis as well as the cells of the diffuse neuroendocrine system (APUD system) and influences the modulation of metabolic processes in the body [7].
Nowadays, there have been several studies, demonstrating the ability of melatonin to alleviate inflammation and the intensity of “cytokine storms” in patients with COVID-19. Melatonin supplements are effective in patients hospitalized with COVID-19 due to decreased vascular permeability, and they can be used in combination with COVID-19 medications and treatments [8]. Therefore, the study of the levels of MT and ST neurotransmitters involved in the regulation of the immune response, resistance to stress, functioning of various organs and systems, especially in patients with comorbid pathology, and namely NAFLD, type 2 diabetes, obesity, is an urgent issue of clinical medicine, especially among individuals infected with COVID-19.
The purpose of the study was to determine the peculiarities of changes in serum melatonin and serotonin neurohormone levels in patients with NAFLD and kidney damage infected with the COVID-19 virus.
Materials and methods
A complex examination of the patients was carried out on the clinical base of the Department of Propaedeutics of Internal Medicine, Faculty of Medicine, State Higher Educational Establishment “UzhNU”. The scientific study included 72 patients with non-alcoholic fatty liver disease (steatohepatitis) combined with increased body mass index (BMI) (overweight or obesity of varying severity) and carbohydrate metabolism disorders, who were treated in the department for COVID-19 infected patients at the CNE “TRCH named after A. Novak” (TRD) from October 2020 to 2022 and had a confirmed diagnosis of COVID-19 pneumonia (positive polymerase chain reaction (PCR test) to SARS-CoV-2 RNA (RdRP SARS-CoV-2 gene, E SARS-CoV-2 gene), as well as “ground-glass opacity” lung lesion on CT scan with a maximum percentage of lung tissue damage up to 65.0 %) and did not require connecting the patients to an artificial lung ventilation apparatus. It was decided to hospitalize these patients due to the high risk of possible complications and a more severe course of viral infection against the background of comorbid pathology. Patients were diagnosed (determination of blood levels of procalcitonin, interleukin-6, C-reactive protein, ferritin, D-dimer) and treated (prescription of antiviral therapy, glucocorticoids, anticoagulants, vitamin D3, zinc medication, and antibiotic therapy) according to the standards of medical treatment for COVID-19 infections. It should be noted that the examined NAFLD patients were not diagnosed with kidney damage before admission to the hospital due to the COVID-19 infection.
Exclusion criteria from the study included an extremely severe condition of patients infected with COVID-19, presence of congenital malformations of the urinary system, acute and chronic glomerulonephritis and pyelonephritis, type 1 diabetes, the presence of alcohol, autoimmune, viral lesions (hepatitis B, C, D viruses) of the liver.
The control group included 20 virtually healthy individuals (12 (60.0 %) were men and 8 (40.0 %) were women. The average age was (49.6 ± 7.1) years).
All studies were performed with the consent of the patients (written consent was obtained from all the patients for the appropriate diagnostic and therapeutic measures), and the methodology was consistent with the Helsinki Declaration of Human Rights, 1975 and its revision of 1983, the Council of Europe Convention on Human Rights and Biomedicine and the legislation of Ukraine.
All examined patients were subjected to investigation by general clinical, anthropometric, instrumental and laboratory methods. To verify the diagnosis, attention was paid to the nature of the complaints and medical history. The anthropometric study involved determining height, weight, waist circumference, and calculating the BMI.
All patients underwent an ultrasound examination of the abdominal cavity and kidneys according to the standard methodology. At the beginning of the inpatient phase of treatment (day 1), as well as on day 10 of inpatient treatment (IT), standard general and biochemical tests were performed in blood serum to determine the functional status of the liver (alanine aminotransferase (ALT), aspartate aminotransferase (AST), total bilirubin (TBL) and its fractions, alkaline phosphatase (ALP), gamma-glutamyltransferase (GGT)), kidneys (creatinine level, urea), lipid and carbohydrate metabolism parameters (glucose, insulin, glycosylated hemoglobin (HbA1c, %), insulin resistance index was calculated (IR-HOMA)). The examined patients were also subjected to cystatin C (CysC) level determination via enzyme multiplied immunoassay using “BioVendor” test system (the Czech Republic).
All examined patients were also tested for melatonin (MT) levels in blood serum via radioimmune analysis and the usage of test systems (LDN Labor Diagnostika Nord GmbH, Germany). Blood sampling was performed at the same time from 7:30 to 8:00 a.m. in both examined patients and healthy individuals in the control group, considering the fact that melatonin levels are related to the circadian biorhythm. Serotonin (ST) levels in blood serum were also determined by high-performance liquid chromatography on an Agoilent 1100 chromatograph, using the Agilent Technologies (USA) test system.
The diagnosis of NAFLD was performed according to the criteria of the unified clinical protocol (Order of the Ministry of Health of Ukraine № 826 dated 06.11.2014) and EASL-EASD-EASO clinical practice guidelines for the diagnosis and treatment of NAFLD [9]. The degree of liver damage was estimated using surrogate markers of fibrosis with the help of online NAFLD fibrosis score (NFS) calculators, Fibrosis 4 calculator (FIB-4), fibrotest, as well as liver elastometry results.
Type 2 DM was diagnosed according to the IDF recommendations (2005), as well as taking into account the criteria of the unified clinical protocol (order of the Ministry of Health of Ukraine No. 1118 of December 21, 2012) [10]. The severity of type 2 DM was assessed by the HbA1c level (the norm is up to 6.0 %).
To research the functional state of the kidneys in the examined patients, the glomerular filtration rate (GFR) was calculated using the creatinine index, the MDRD (Modification of Diet in Renal Disease) formula and the Cockroft-Gault (CG) formula [11] as well as the formula in which the cystatin C level was applied (GFRCysС = 94,652 × Cys С–1,2478) [12].
NAFLD patients were divided into two groups depending on the presence or absence of type 2 DM, and namely:
— Group 1 included 34 NAFLD and insulin resistance (IR) patients (19 (55.9 %) were men, 19 (44.1 %) were women; the average age was (51.7 ± 4.8) years);
— Group 2 comprised 38 patients with NAFLD and type 2 DM (among them 22 (57.9 %) were men and 16 (42.1 %) were women; the average age was (50.2 ± 5.3) years).
The results of the patients’ examination were analyzed and processed using the computer program Statistica 10.0 (StatSoft Inc., USA) applying parametric and nonparametric methods of assessing the results.
Results
All patients under our observation were diagnosed with NAFLD, namely, non-alcoholic steatohepatitis of minimal degree of activity at the time of their admission to the hospital. At the same time, more pronounced changes in transaminase levels at the time of admission for inpatient treatment were diagnosed in group 2 patients. On day 10 of IT, all the patients with COVID-19 infection were diagnosed with increased activity of liver transaminases, as well as total bilirubin level, which, in our opinion, is connected with the toxic influence of prescribed therapy on the patients’ compromised liver, which is confirmed by the increase in GGT level (Table 1).
/41.jpg)
The determination of carbohydrate metabolism indices confirms type 2 DM in group 2 patients and IR in patients examined in group 1 at the time of admission for IT due to COVID-19 infection. The aggravation of acute respiratory infection, as well as the prescription of glucocorticoid drugs to stabilize the patients’ condition, contributed to the increase in blood sugar levels in both examined groups, as well as the progression of hyperinsulinemia in Group 1 patients. Group 2 patients demonstrated a tendency to decrease insulin and C-peptide activity in blood serum on day 10 of IT (Table 2).
/42.jpg)
At the beginning of the inpatient phase of treatment in the COVID-19-infected patients that we examined, the indicators of renal functional status did not indicate its impairment in patients with NAFLD in combination with IR or type 2 DM. On day 10 of IT, these patients had increased serum creatinine and urea levels, as well as proteinuria and decreased GFR, indicating renal damage against the background of COVID-19 infection. At the same time, the daily proteinuria in patients of both groups differed from that of the control group at the time of admission to the hospital and increased to a maximum of (367.0 ± 2.8) mg/day on the 10th day of IT (p < 0.05) in Group 2 patients (Table 3). All examined patients in both groups also demonstrated erythrocyturia and leukocyturia against the background of COVID-19 infection, which increased progressively by day 10 of IT.
On day 10 of IT, the determination of GFR revealed a decrease in the filtration capacity of the kidneys in both groups of patients, regardless of the method of its calculation. Consequently, in NAFLD patients with impaired carbohydrate metabolism, acute respiratory infection COVID-19 contributes to the formation of kidney damage.
There was a significant decrease in serum MT level in both examined groups — by 2.2 and 3.2 times respectively in group 1 and 2 patients at the time of admission to the hospital. The same trend was identified in the indicators of serum MT level in both groups of patients on day 1 of IT — and namely, its decrease by 1.5 and 2.3 times. Both MT and ST levels progressively decreased on day 10 of treatment for COVID-19 infection in NAFLD patients combined with carbohydrate metabolism disorders (Table 4).
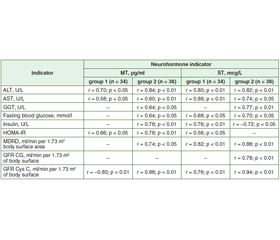
We analyzed the relationship between the decrease in serum neurohormone levels and the indicators of the functional state of the liver and kidneys, and carbohydrate metabolism in the patients on day 10 of inpatient treatment (Table 5).
/43.jpg)
Statistical analysis revealed a correlation between the progression of liver damage and the decrease of MT and ST levels in blood serum, which is probably a consequence of its toxic damage against the background of the conducted treatment of patients infected with COVID-19. The decreased serum neurohormone levels also correlate with the insulin level and insulin resistance index. There is also a strong correlation between renal damage occurring at the IT stage in NAFLD patients and impaired carbohydrate metabolism during COVID-19 infection and decreased levels of MT and ST in the blood, according to GFR MDRD. A more pronounced correlation between changes in the functional state of the kidneys and neurohormone indicators was established in group 2 patients (NAFLD in combination with type 2 diabetes mellitus) mainly when determining GFR by the Cys C index.
Discussion
The study of the influence of neurotransmitters (MT, ST) on the formation of lesions of various organs and systems during COVID-19 infection is of particular interest, especially in patients with metabolically associated diseases, such as NAFLD, type 2 diabetes, obesity, etc.
The experimental study (Kolyanyk I.A., Herush I.V., 2020) revealed an imbalance of antioxidant system parameters when modelling nephropathy with folic acid, which is probably due to increased free-radical damage to biomolecules. The administration of melatonin for 7 days contributes to the normalization of indicators of the antioxidant system in the liver of rats with nephropathy, which is due to its ability to directly neutralize toxic compounds and activate antioxidant enzymes [13]. Another experimental study (Kryvchanska M.I. et al., 2016) also studied the effect of melatonin on the correction of disorders of circadian organization of renal function and deviations of the morphological state of the kidneys caused by propranolol. The studies suggest that exogenous melatonin is able to influence the indicators of the main renal functions, demonstrating a pleiotropic effect [14].
Clinical studies based on the determination of melatonin concentrations in patients with different degrees of renal dysfunction in chronic kidney disease revealed a correlation between total melatonin concentration and GFR. A decrease in melatonin concentration and a disruption in its synthesis rhythm occurred in accordance with the progression of renal dysfunction. In experimental animal models in the formation of pyelonephritis, renal failure, arterial hypertension and diabetes mellitus, a decrease in the severity of oxidative stress, inhibition of chronic inflammation and limitation of apoptosis with increasing concentrations of melatonin were demonstrated. The administration of exogenous melatonin promotes a decrease in urine osmolarity, urinary concentration of sodium and potassium ions, and an increase in GFR. All these effects are associated with a decrease in parenchymal cell damage, fibrosis and the decrease in proteinuria under the influence of melatonin [15].
The important role of ST in the regulation of circadian rhythm of renal function has also been proved [16]. In the experiment serotonin administration under conditions of bilateral vagotomy promotes the restoration of the organ blood supply, including glomeruli and tubules, prevents the development of proximal tubule epithelium necrosis. Thus, the activation of the serotonergic system can compensate for the impaired parasympathetic innervation of the kidney [17].
The findings we obtained indicate the decrease of serum MT and ST levels in NAFLD patients and impaired carbohydrate metabolism with the most pronounced deviation from the norm in NAFLD patients with type 2 diabetes mellitus. Impaired renal function developed in the patients with COVID-19 infection, as well as due to its therapy, contributes to an even more progressive decrease in these neurohormones in the blood serum. A direct correlation was established between the decreased serum levels of ST and MT and the decreased FFR (especially according to the level of Cys C). It is suggested that endogenous administration of MT and/or ST to NAFLD patients (especially in combination with type 2 DM), when infected with COVID-19, may improve the functional ability of organs and body systems, including the kidneys. However, further studies in this direction are required for more specific conclusions.
Conclusions
1. COVID-19 infection and its treatment in NAFLD patients with impaired carbohydrate metabolism lead to impaired renal functional status.
2. In patients with NAFLD and carbohydrate metabolism disorders, a decrease in serum levels of the neurohormones melatonin and serotonin was found, which progressively decreased against the background of COVID-19 infection and kidney damage in these patients.
Received 05.01.2022
Revised 11.01.2022
Accepted 18.01.2022

/41.jpg)
/42.jpg)
/43.jpg)