Introduction
Irritable bowel syndrome (IBS) is a common disorder of the gastrointestinal tract with unclear etiology and no reliable biomarker. Like other chronic and functional disorders, medical treatments for IBS are suboptimal and the overall illness burden is high. Patients with IBS report high rates of psychopathology, low quality of life, and increased suicidal ideation. These patients also miss more days of work, are less productive at work, and use many healthcare resources. However, little is known about the burden of IBS on daily functioning [1].
Psychological stress is an important factor for the development of IBS. More and more clinical and experimental evidence showed that IBS is a combination of irritable bowel and irritable brain. Evidence from clinical and experimental studies showed that psychological stresses have marked impact on intestinal sensitivity, motility, secretion and permeability, and the underlying mechanism has a close correlation with mucosal immune activation, alterations in central nervous system, peripheral neurons and gastrointestinal microbiota. Stress-induced alterations in neuro-endocrine-immune pathways acts on the gut-brain axis and microbiota-gut-brain axis, and cause symptom flare-ups or exaggeration in IBS. IBS is a stress-sensitive disorder, therefore, the treatment of IBS should focus on managing stress and stress-induced responses. Now, non-pharmacological approaches and pharmacological strategies that target on stress-related alterations, such as antidepressants, antipsychotics, miscellaneous agents, 5-HT synthesis inhibitors, selective 5-HT reuptake inhibitors, and specific 5-HT receptor antagonists or agonists have shown a critical role in IBS management. A integrative approach for IBS management is a necessary [2].
The current goal of treatment in irritable bowel syndrome focuses primarily on symptom management and attempts to improve quality of life. Several treatments are at the disposal of physicians; lifestyle and dietary management, pharmacological treatments and psychological interventions are the most used and recommended. Psychological treatments have been proposed as viable alternatives or compliments to existing care models. Most forms of psychological therapies studied have been shown to be helpful in reducing symptoms and in improving the psychological component of anxiety/depression and health-related quality of life. According to current NICE/NHS guidelines, physicians should consider referral for psychological treatment in patients who do not respond to pharmacotherapy for a period of 12 months and develop a continuing symptom profile (described as refractory irritable bowel syndrome). Cognitive behavioral therapy is the best studied treatment and seems to be the most promising therapeutic approach. However, some studies have challenged the effectiveness of this therapy for irritable bowel syndrome. One study concluded that cognitive behavioral therapy is no more effective than attention placebo control condition and another study showed that the beneficial effects wane after six months of follow-up. A review of mind/body approaches to irritable bowel syndrome has therefore suggested that alternate strategies targeting mechanisms other than thought content change might be helpful, specifically mindfulness and acceptance-based approaches [3]. Thus, the study of mental health in patients with IBS is a promising area of medicine not only in terms of determining the psychological profile, but can also serve as an alternative in terms of further management and treatment of this group of patients.
The purpose of the study was to examine mental health of IBS patients.
Materials and methods
54 patients with IBS were examined in the psychiatric clinic of Gǟvle Hospital in 2019–2021. They were included in group I of the examined patients that consisted of 42 females (77.8 %) and 12 males (22.2 %) with the mean age of 31.2 ± 4.8 years. The control group (group II) included 40 healthy individuals: 31 females (77.5 %) and 9 males (22.5 %) with the mean age of 30.9 ± 5.1 years.
All studies were performed with the consent of patients (all patients gave their written consent for appropriate diagnostic and treatment procedures), and the methodology was in accordance with the Helsinki Declaration of Human Rights of 1975 and its revision in 1983, the Council of Europe Convention on Human Rights and Biomedicine, and Swedish legislation.
Before conducting the survey, the patients were informed about the filling technique and the survey started only when they made certain that they understood this technique correctly. Assessment of the psychological status was determined using the following methods:
1. Psychological Stress Measure PSM-25 by Lemyr-Tessier-Fillion. The method was first developed in France, then adopted and validated in Great Britain, Spain and Japan. It aims to assess the level of stress in somatic, behavioral and emotional scores. It consists of a number of questions characterizing mental. The patient needs to estimate the condition for the last week by an 8-point scale. To do this, they have to circle the number from 1 to 8 next to each statement, which most accurately identifies the experience. Numbers from 1 to 8 indicate the frequency of experiences: 1 — “never”; 2 — “extremely rarely”; 3 — “very rarely”; 4 — “rarely”; 5 — “sometimes”; 6 — “frequently”; 7 — “very frequently”; 8 — “constantly (daily)”. The sum of all answers is calculated to obtain the integral psychological stress measure (PSM). Question 14 is evaluated in reverse order. The higher the PSM, the higher the level of psychological stress. PSM of more than 155 points indicates a high level of stress, a state of maladaptation and mental discomfort, the need to use a wide range of tools and methods to reduce mental stress, psychological relief, change the way of thinking and living. PSM in the range of 100–154 points shows the average level of stress. PSM less than 100 points, indicates a low level of stress and the state of psychological adaptation to workload [4].
2. The Holmes and Rahe Stress Scale. It consists of a scale that includes 43 questions about important life events (Life Change Units), each corresponding to a certain number of points depending on the degree of its stressfulness. A large number of points scored, i.e. 300 or more is an alarm that warns of the risk of psychosomatic diseases. Thus, the total score of 150–199 means the degree of stress resistance is high, 200–229 points is the threshold, and 300 or more points means low degree [5].
3. Health Assessment 36-Item Short Form Survey (SF-36 Health Assessment). This is a non-specific questionnaire for assessing the quality of life of a patient with various chronic diseases, which is widely used in quality of life studies in Europe and the United States. The questionnaire reflects the general well-being and satisfaction of those aspects of human life that are affected by health. SF-36 consists of 36 questions grouped into eight scales: physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional and mental health. The indicators of each scale are compiled in such a way that the higher the value of the indicator (from 0 to 100), the better the score on the selected scale. They form two summary scores: mental component summary and physical components summary of health. Data processing is carried out using special formulas to calculate the value of each score, and then summarizes the two main parameters — mental and physical components of health [6].
The analysis and processing of the results of the examination of patients was performed using the computer program Statistics for Windows v. 10.0 (StatSoft Inc., USA) by parametric and non-parametric methods of evaluation of the results.
Results
Despite the fact that physical symptoms (abdominal pain, intestinal spasm, defecatory dysfunction) were the main complaints in the clinical picture of our patients with IBS, it was found that the key factor in exacerbating and maintaining IBS physical symptoms are psychosocial (cognitive and emotional) factors. Most of the examined patients reported experiences such as anxiety about their symptoms, their consequences and duration, anxiety, depression, stress, shame and anger. Among these psychosocial factors, the so-called gastrointestinal specific anxiety was most often identified. This was defined as “a cognitive, affective and behavioral response that results from a fear of gastrointestinal sensations, symptoms and the context in which these visceral sensations, pain and symptoms occur”.
We evaluated the quality of life and psychological state of the examined patients with IBS. Analyzing the PSM-25 questions answered by patients from group I with IBS (n = 54) and from control group II (n = 40) on the level of psychological stress, the following results were obtained with gender distribution: 42.9 % of female patients of group I had a high level of stress, and 50.0 % a medium level of stress; low levels of stress were found in only 7.1 % of female patients of group I. 25.8 % of the surveyed females of the control group II had a medium level of stress, and 74.2 % had a low level of stress (fig. 1).
As for male patients, the following results were obtained: 66.7 % of male patients of group I had a high level of stress, and 33.3 % an average level of stress.77.8 % of the surveyed males of the control group had a low level of stress and 22.2 % had a medium level of stress (fig. 2).
It should also be noted that among male IBS patients from group I significantly higher levels of stress were found more often than in female patients from the same group, where a medium level of stress was more often found. Among both females and males of the surveyed control group a low level of stress was significantly more frequently found (fig. 3).
After analyzing the level of stress, we assessed stress resistance, as a significant proportion of patients showed high and medium levels of stress. For this purpose we used the Holmes-Rahe survey. The analysis of the survey of group I patients with IBS and control group II of healthy subjects gave the following results: among females, namely in female patients of the group I threshold stress resistance was more often observed (57.1 % of patients); 42.9 % of patients had a low level of stress resistance. The survey of the control group II showed slightly different results. Thus, 83.9 % of females surveyed showed a high level of stress resistance, while only 16.1 % of patients showed threshold stress resistance (fig. 4).
/47.jpg)
In the analysis of the Holmes-Rahe survey in group I patients with IBS and control group II we obtained the following results: males with IBS often had a low level of stress resistance (58.3 % of patients), while 41.7 % had threshold stress resistance. The survey of the control group II had slightly different results. Thus, 66.7 % of surveyed men of the II group showed a low level of stress resistance, while only 33.3 % of respondents in the same group showed threshold stress resistance.
According to the data, high and threshold levels of stress resistance were found among group I patients of both sexes.
To assess the quality of life, all subjects completed the SF-36 questionnaire, and the main scores of physical and mental health of patients were derived based on the analysis. The following scores of the psychological component of health in patients of group I with IBS were obtained: psychological health — (32.7 ± 0.9), role emotional — (10.6 ± 1.1), social functioning — (43.7 ± 1.4), and viability — (23.5 ± 0.9). The results indicate a relatively low level of the psychological component of health and in turn indicates a rather reduced quality of life of patients.
The following scores of the psychological component of health were obtained in the subjects of the control group II, namely: psychological health — (85.6 ± 1.7), role emotional — (79.6 ± 1.5), social functioning — (86.6 ± 1.4), and viability — (78.9 ± 1.1). The results indicate a relatively high level of the psychological component of health.
The following scores of the physical component of health in patients of group I with IBS were obtained: general health — (30.9 ± 1.7), bodily pain — (40.2 ± 0.8), role physical — (25.5 ± 1.4), and physical functioning — (38.9 ± 0.9). The results testify to rather low level of the physical component of health and in turn indicates rather reduced quality of life of patients.
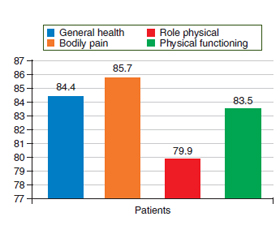
The following scores of the physical component of health in the surveyed control group II were obtained: general health — (84.4 ± 1.6), bodily pain — (85.7 ± 0.9), role physical — (79.9 ± 1.4), and physical functioning — (83.5 ± 1.7). The results show a fairly high level of the physical component of health and in turn indicates a fairly high quality of life of the subjects.
Thus, the level of stress was significantly higher in patients with IBS compared with the control group II. According to the survey on the psychological and physical component of health, these scores were also reduced in patients with IBS compared with the control group.
Discussion
Although IBS is not fully understood, symptoms appear to result from a disturbance in the brain-gut axis — the line of communication that exists between the brain and the gastrointestinal tract that may include disruptions in the microbiome and the immune system. This helps explain why approximately half of all IBS patients, particularly those who suffer from chronic abdominal pain, report mental symptoms and distress along with abnormal and inexplicable symptoms that were once considered to be “all in their heads” because doctors couldn’t find any physical abnormalities.
The frequent co-occurrence of irritable bowel syndrome and the common mental disorders of anxiety and depression is well established. A range of biological and psychosocial disease mechanisms are common to both disorders, many of which contribute to a dysregulated gut — brain axis. Clinical and subthreshold psychological comorbidity adds to the functional impairment and disease burden in individuals with irritable bowel syndrome. Progress is being made with regard to understanding irritable bowel syndrome in the clinical setting from a biopsychosocial perspective. However, until now, most trials of irritable bowel syndrome treatment still consider the disease as a gut disorder in isolation, which leaves major gaps in knowledge about disease — disease interactions and treatment outcomes in irritable bowel syndrome [7].
Jeffrey M. Lacner and co-authors studied comorbidity in patients with IBS, while detailing the nature of physical and mental comorbidities among the cohort of patients with IBS. The study assessed how comorbidity affects their daily lives, determining the specific conditions of coexistence, both individually and in combination, most strongly associated with worsening symptoms of the gastrointestinal tract, mental and physical functioning, and quality of life [8].
/48_2.jpg)
Another study evaluated the prevalence of anxiety and depressive symptoms and disorders in patients with IBS. It showed that the risk of these psychiatric problems is significant and found significantly higher levels of anxiety (SMD = 0.76) and depression (SMD = 0.80) in patients with IBS compared with the control group of healthy individuals. Systematic review of Li et al., which included 27 studies, similarly indicated that anxiety levels (SMD = 0.84) and depression (SMD = 0.76) were significantly higher in patients with IBS than in healthy subjects. The authors concluded that in patients with IBS, the degree of anxiety and depression is explained by the “brain-intestine” interaction. This is evidenced by psychophysiological dysfunctions of the brain-gut axis, which is a bidirectional neurological system between the brain and the digestive system, which leads to the appearance of IBS symptoms. According to this model, abdominal symptoms affect anxiety and depression, and, on the other hand, the psyche, and these factors exacerbate mental disorders. It is recommended that these comorbid psychosomatic illnesses be systematically assessed and treated in patients with IBS. In addition, it is recommended that physicians who treat patients with anxiety and depression also evaluate them for IBS [9].
The results of our research also indicate a decrease in the physical and mental components of health in the examined patients with IBS. These changes occur against the background of reduced stress resistance and increased body response to stressful situations, especially in female patients. According to their own experience, patients with IBS tend to avoid situations that they have ever associated with symptoms of IBS (certain foods or social work-related situations, such as meetings or gatherings). However, they also limit themselves in certain social situations, such as leisure or travel, personal and intimate relationships. Although most patients believe that this type of reaction is important for the treatment of their condition, they also recognize that it is the main cause of their suffering and reduced quality of life.
Thus, according to our data, which also coincide with the opinion of other scientists, psychological disorders of the gastrointestinal tract is one of the important and still unresolved problems of medicine [10]. An important link between socio-economic factors and psychological disorders in patients with IBS has been shown, which indicates that the treatment strategy requires a combination of efforts of different specialists, namely gastroenterologists, therapists, psychoneurologists and psychiatrists to achieve the maximum therapeutic effect in this group of patients.
Conclusions
1. High and medium levels of stress, as well as reduced stress resistance, were found in IBS patients, which is more pronounced in male patients.
2. Decreased psychological and physical components of health have been found in IBS patients, indicating a reduction in the quality of life of these patients.
Received 02.11.2021
Revised 17.11.2021
Accepted 23.11.2021

/47.jpg)
/48.jpg)