
Журнал "Гастроэнтерология" Том 53, №4, 2019
Вернуться к номеру
Асоціація синдрому надмірного бактеріального росту i неалкогольної жирової хвороби печінки в дітей
Авторы: Yu.M. Stepanov, N.Yu. Zavhorodnia, O.Yu. Lukianenko, E.V. Zygalo, V.B. Yagmur
State Institution “Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine”, Dnipro, Ukraine
Рубрики: Гастроэнтерология
Разделы: Медицинские форумы
Версия для печати
Актуальність. Неалкогольна жирова хвороба печінки (НАЖХП) посiдає провідні позиції серед хронічних захворювань печінки в дітей у промислово розвинених країнах. Відомо, що для пацієнтів iз НАЖХП характерна висока поширеність синдрому надмірного бактеріального росту (СНБР). Метою роботи є вивчення впливу СНБР на структурно-функціональні показники печінки в дітей iз надмірною вагою та ожирінням. Матеріали та методи. Обстежено 73 дитини віком від 6 до 17 років, середній вік пацієнтів становив (11,41 ± 2,68) року. Залежно від наявності надмірної ваги/ожиріння i результатів водневого дихального тесту (ВДТ) з глюкозою пацієнти були розподілені на 2 групи: 1 група — 30 дітей iз надмірною вагою/ожирінням та СНБР, 2 група — 28 дітей iз надмірною вагою/ожирінням без СНБР. Контрольну групу становили 15 практично здорових дітей iз нормальною вагою та без СНБР за результатами ВДТ з глюкозою. Наявність стеатозу печінки встановлювали за допомогою транзієнтної еластографії з функцією САР. Додатково проводили ВДТ з лактозою та біохімічний аналіз крові з визначенням показників біохімічної гепатограми, ліпідного й вуглеводного спектрів. Результати. Встановлено, що в 70 % дітей 1 групи була супутня НАЖХП порівняно з 32 % у 2 групі. У 1 групі швидкість осідання еритроцитів була вищою, ніж у 2 і 3 групах (p < 0,05). Також у дітей 1 групи рівні тригліцеридів і ліпопротеїнів дуже низької щільності були в 1,5 раза вищими. Відмічено тенденцію до більш високих значень інсуліну та індексу НОМА в 1 групі порівняно з другою. Мальабсорбцію лактози діагностовано в 17 (56,7 %) дітей iз НАЖХП, лактозозалежний СНБР — у 15 (50,0 %). При ожирінні без НАЖБП мальабсорбцію лактози виявлено в 10 (35,7 %) пацієнтів, а лактозозалежний СНБР — у 9 (32,1 %). Таким чином, у дітей iз НАЖХП мальабсорбція лактози зустрічалася в 1,6 раза частіше, ніж у дітей без НАЖБП. Висновки. Встановлено, що НАЖХП є фактором ризику формування СНБР. СНБР асоційований з низькорівневим запаленням, діти з СНБР на тлі ожиріння характеризувалися більш несприятливим метаболічним профілем у вигляді змін параметрів ліпідного і вуглеводного обміну, що може призводити до прогресування НАЖХП. Продемонстровано високу частоту мальабсорбції лактози і лактозозалежного СНБР у дітей iз НАЖХП.
Актуальность. Неалкогольная жировая болезнь печени (НАЖБП) занимает лидирующие позиции среди хронических заболеваний печени у детей в промышленно развитых странах. Известно, что для пациентов с НАЖБП характерна высокая распространенность синдрома избыточного бактериального роста (СИБР). Цель работы — изучить влияние СИБР на структурно-функциональные показатели печени у детей с избыточным весом и ожирением. Материалы и методы. Обследовано 73 ребенка в возрасте от 6 до 17 лет, средний возраст пациентов составил (11,41 ± 2,68) года. В зависимости от наличия избыточного веса/ожирения и результатов водородного дыхательного теста (ВДТ) с глюкозой пациенты были разделены на 2 группы: 1 группа — 30 детей с избыточным весом/ожирением и наличием СИБР, 2 группа — 28 детей с избыточным весом/ожирением без СИБР. Контрольную группу составили 15 практически здоровых детей с нормальным весом и без СИБР по результатам ВДТ с глюкозой. Наличие стеатоза печени устанавливали при помощи транзиентной эластографии с функцией САР. Дополнительно проводили ВДТ с лактозой и биохимический анализ крови с определением показателей биохимической гепатограммы, липидного и углеводного спектров. Результаты. Установлено, что 70 % детей 1 группы имели сопутствующую НАЖБП по сравнению с 32 % во 2 группе. В 1 группе скорость оседания эритроцитов была выше, чем во 2 и 3 группах (p < 0,05). Также у детей 1 группы уровни триглицеридов и липопротеинов очень низкой плотности были в 1,5 раза выше. Отмечена тенденция к более высоким значениям инсулина и индекса НОМА в 1 группе по сравнению со второй. Мальабсорбция лактозы диагностирована у 17 (56,7 %) детей с НАЖБП, лактозозависимый СИБР — у 15 (50,0 %). При ожирении без НАЖБП мальабсорбция лактозы выявлена у 10 (35,7 %) пациентов, а лактозозависимый СИБР — у 9 (32,1 %). Таким образом, у детей с НАЖБП мальабсорбция лактозы встречалась в 1,6 раза чаще, чем у детей без НАЖБП. Выводы. Установлено, что НАЖБП является фактором риска формирования СИБР. СИБР ассоциирован с низкоуровневым воспалением, дети с СИБР на фоне ожирения характеризовались более неблагоприятным метаболическим профилем в виде изменений параметров липидного и углеводного обмена, что может приводить к прогрессированию НАЖБП. Продемонстрирована высокая частота мальабсорбции лактозы и лактозозависимого СИБР у детей с НАЖБП.
Background. Non-alcoholic fatty liver disease (NAFLD) is a leading etiological factor of chronic liver diseases in children in industrialized countries. The high prevalence of small intestinal bacterial overgrowth (SIBO) is common in patients with NAFLD. Therefore, the purpose of our work is to study the impact of SIBO on the structural and functional parameters of the liver in obese/overweight children. Materials and methods. We examined 73 children aged 6 to 17 years, mean age of patients was (11.41 ± 2.68) years. Depending on the presence of overweight/obesity and the results of glucose hydrogen breath test (HBT), patients were divided into 2 groups: group 1 — 30 overweight/obese persons with SIBO, group 2 — 28 overweight/obese children without SIBO. The control group consisted of 15 apparently healthy children with normal weight and without SIBO. The presence of liver steatosis was established by means of transient elastography with controlled attenuation parameter. Additionally, we performed lactose HBT and a biochemical blood test with biochemical hepatogram, determination of lipid and carbohydrate parameters. Results. It was found that 70 % of children in group 1 had NAFLD, compared to 32 % in group 2. Also, erythrocyte sedimentation rate was higher in group 1 than in groups 2 and 3 (p < 0.05). Patients of group 1 had 1.5 times higher levels of triglycerides and very low-density lipoproteins. There was a tendency towards higher values of insulin and homeostatic model assessment in group 1 compared to group 2. Lactose malabsorption was diagnosed in 17 (56.7 %) children with NAFLD, lactose-dependent SIBO — in 15 (50.0 %). Among obese patients without NAFLD, lactose malabsorption was found in 10 (35.7 %) cases, and lactose-dependent SIBO — in 9 (32.1 %). Thus, in children with NAFLD, lactose malabsorption was detected 1.6 times more frequently than in children without NAFLD. Conclusions. It has been found that NAFLD is a risk factor for SIBO development. SIBO was associated with low-grade inflammation and adverse metabolic profile. The high frequency of lactose malabsorption and lactose-dependent SIBO among children with NAFLD was demonstrated.
неалкогольна жирова хвороба печінки; діти; синдром надмірного бактеріального росту; мальабсорбція лактози
неалкогольная жировая болезнь печени; дети; синдром избыточного бактериального роста; мальабсорбция лактозы
non-alcoholic fatty liver disease; children; small intestinal bacterial overgrowth syndrome; lactose malabsorption
Introduction
The global epidemic of obesity has led to changes in the etiological structure of the digestive system diseases. So, at the present time, non-alcoholic fatty liver disease (NAFLD) is a leader among chronic liver diseases in children in industrialized countries [8]. NAFLD is considered as a liver manifestation of metabolic syndrome and includes a wide pathological spectrum, ranging from simple steatosis to a different degree of necrotic inflammation (non-alcoholic steatohepatitis), which leads to the development of fibrosis, and subsequently to liver cirrhosis. Recent studies suggest that NAFLD should be considered as multisystem disease [1], because this condition is associated with a range of extrahepatic pathologies such as atherosclerosis, type 2 diabetes, osteopenia, obstructive sleep apnea syndrome, and the like [4].
It is known that there is a high prevalence of small intestinal bacterial overgrowth (SIBO) syndrome in NAFLD patients [10]. SIBO is defined as an increase in the number of bacteria (over 105 CFU/ml) in the proximal small intestine. The gold diagnostic standard for SIBO is a bacteriological examination of the aspirate from the proximal part of small intestine. However, this method is invasive and has a number of limitations, therefore, most diagnoses are based on glucose or lactose hydrogen breath test (HBT). In accordance with the Rome criteria on the use of HBT, glucose HBT is the most accurate method for non-invasive diagnosis of SIBO [11]. SIBO and increased intestinal permeability are considered as the main mechanisms for the translocation of bacteria and their products, which can contribute to a cascade of adverse events such as oxidative stress, insulin resistance, inflammation and liver fibrosis [14].
Most of the works investigating SIBO effect on NAFLD development was performed in adult patients [9, 10, 14, 16, 18, 20]. Frequently, for the diagnosis of SIBO, glucose hydrogen breath test is used, data on the presence of lactose-dependent SIBO in such patients are limited.
Therefore, the purpose of our work is to study the influence of SIBO and features of lactose digestion on structural and functional parameters of the liver in obese/overweight children.
Materials and methods
A total of 73 children aged 6 to 17 years underwent treatment at the Pediatric Gastroenterology Department of the Institute of Gastroenterology of the National Academy of Medical Sciences of Ukraine in 2017–2018. The average age of patients was (11.41 ± 2.68) years. Before the study, the parents and patients were fully informed about the methods and amount of the research and gave consent for the planned studies. Clinical examination of patients, anthropometry with subsequent calculation of body mass index (BMI) [13] were performed. The presence of obesity/overweight was determined according to the World Health Organization recommendations [13]. The presence of abdominal obesity was diagnosed with a waist circumference (WC) measurement according to the recommendations of the International Diabetes Federation [17].
All the patients underwent a general blood test and a biochemical blood test with determination of the levels of total protein, total bilirubin, alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma-glutamyl transpeptidase (GGT) using the biochemical analyzer Stat Fax 1904 Plus (Awareness Technology, USA). For the biochemical study of blood lipids, the content of total cholesterol (TC), triglycerides (TG), high-density lipoprotein (HDL) cholesterol using Cormay reagents (Poland) was determined using the same analyzer with the subsequent calculation of low-density lipoprotein (LDL) and very low-density lipoprotein (VLDL) cholesterol.
The content of insulin in the blood serum was determined by the immunogenic enzyme test method (DRG International, Inc., Germany) using Stat Fax 303 Plus (USA) reader. Then, the homeostasis model assessment (HOMA) was calculated. The level of glycosylated hemoglobin was measured using a spectrophotometer SF-4 (Lachema).
Glucose tolerance was evaluated on the basis of the oral glucose tolerance test (OGTT). Glucose loading was carried out at the rate of 1.75 g per 1 kg of body weight (not more than 75 g). In the future, hyperglycemic and hypoglycemic factors were calculated.
Diagnosis of SIBO was determined from glucose HBT data using the Gastro+ Gastrolyzer gas analyzer (Bedfont Scientific Ltd, UK). The dose of glucose was 1 g per 1 kg of body weight, but not more than 50 g, dissolved in 250 ml of water. The HBT result was assessed as positive for SIBO if hydrogen concentration has increased for more than 10 parts per million (ppm). For the diagnosis of lactose malabsorption and lactose-dependent SIBO, lactose HBT was performed at the rate of 1 g per 1 kg of body weight (not more than 25 g) dissolved in 10 ml of warm water per 1 kg of body weight, but not more than 250 ml. An increase in hydrogen content for more than 10 ppm from baseline during the first 30–60 minutes indicated lactose-dependent SIBO. Absolute and relative contraindications to HBT were taken into account. For the diagnosis of liver steatosis, transient elastography was performed using the FibroScan® 502 touch (Echosens, Paris, France) with the controlled attenuation parameter (CAP). Diagnosis of NAFLD was established according to CAP and exclusion of secondary steatosis in children with overweight/obesity. Liver stiffness was evaluated in kilopascals (kPa), degree of viscosity, or fatty degeneration, — in decibels per meter (dB/m). To establish the diagnosis and assess the severity of disease, we used unified clinical protocols [2].
Statistical processing of research results was carried out using the methods of variation statistics implemented by the standard package of applications Statistica 7.0 for Windows. The normality of the distribution of characteristics was checked out using Shapiro-Wilk test. Depending on the distribution of signs, quantitative data were presented in the form of mean and standard deviations (M ± SD) or in the form of medians and interquartile intervals (Me [25; 75 %]), for qualitative characteristics — in the form of relative indices (n (%)). The difference in likelihood was based on Mann-Whitney U test and Student’s t-test under normal distribution. When comparing qualitative indicators, the assessment of the likelihood of differences was carried out according to Fisher’s exact test. The ratio of the factor being analyzed to the risk factors was determined on the basis of odds ratio (OR) and relative risk (RR) calculation. The conclusion about the statistical significance of the revealed relationship between the factor and the result was made when the confidence interval did not include 1, that is, both values of the boundaries were either above or below 1. The significance of the differences was set at p < 0.05.
Depending on the presence of overweight/obesity and the results of glucose-based hydrogen breath test, patients were divided into 2 groups: group 1 — 30 overweight/obese children with SIBO, group 2 — 28 overweight/obese children without SIBO. The control group consisted of 15 healthy children with normal weight and no SIBO according to glucose HBT.
Results
Age, sex and anthropometric parameters
The children of the studied groups were homogeneous in terms of the age and sex distribution (Table 1). The analysis of anthropometric data showed that children of groups 1 and 2 did not differ significantly in BMI and WC. In group 1, 21 (70.0 %) patients had obesity, 9 (30.0 %) — overweight; in group 2 — 18 (64.3 %) and 10 (35.7 %) individuals, respectively. The frequency of abdominal type of fat distribution was 83.3 % (25 children) in group 1 and 75.0 % (21 persons) in group 2.
Clinical data
The analysis of complaints showed that children of group 1 more often had diarrhea (an increase in bowel movements to 3 and more times a day) compared to patients of groups 2 and 3 (p < 0.05) (Table 2). Frequency of complaints for flatulence was not significantly different between groups. In group 1, painful palpation in the hypogastrium was twice more likely — 50 compared to 25 % in group 2.
Clinical data of patients, in particular the characteristics of pain syndrome, were mainly due to the concomitant pathology of the digestive system. Characteristics of concomitant pathology are presented in Table 3. A higher frequency of NAFLD and biliary tract disorders in children of group 1 compared to those of groups 2 and 3 (p < 0.05) and a tendency to a higher incidence of gastroesophageal reflux disease in group 1 should be noted.
/63-1.jpg)
General clinical and biochemical tests
The study of general blood test data demonstrated that children of group 1 were characterized by a significantly higher erythrocyte sedimentation rate (ESR) compared to the patients of groups 2 and 3 (p < 0.05) (Table 4). Children with obesity/overweight (groups 1 and 2) were found to be different from those with normal weight with higher ALT and AST (p < 0.05) based on the findings of biochemical functional test.
/63-2.jpg)
Indicators of lipid and carbohydrate spectrum
When studying the parameters of lipid spectrum, it was found that patients with SIBO differed significantly in terms of the higher levels of TG and LDL compared to children without SIBO (p < 0.05) (Table 5). Hypertriglyceridemia was observed in 6 (20 %) persons in group 1 and in 3 (10.7 %) children in group 2. Patients of groups 1 and 2 were also characterized by a lower level of HDL and a higher level of LDL compared to those in group 3 (p < 0.05). The level of insulin and HOMA reached the maximum values in group 1, significantly differing from the corresponding indicators of group 3 (p < 0.05), and showed a tendency to a higher level compared to group 2 (p = 0.06 and p = 0.08, respectively). The increase in HOMA was found in 19 (66.3 %) children in group 1 and in 15 (53.6 %) in group 2. The analysis of OGTT data showed that patients of group 1 differed in terms of higher hyperglycemic coefficient compared to children of groups 2 and 3 (p < 0.05).
Data of instrumental methods
The analysis of transient elastography data demonstrated that children of the first group had higher CAP than those in groups 2 and 3 (p < 0.05) (Table 6). The frequency of liver steatosis among patients in group 1 was 70 % (21 children) compared to 32 % (9 persons) in group 2 (p < 0.05). The stiffness of the liver parenchyma did not differ significantly between the groups.
/64-1.jpg)
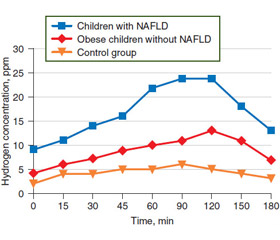
As expected, children of group 1 were characterized by higher levels of hydrogen 60 minutes after glucose loading (Table 6). They also had higher hydrogen concentration 30 and 120 min after lactose loading compared to similar indices in groups 2 and 3 (p < 0.05). When analyzing the data of lactose HBT, it was found that 2/3 of children in group 1 and 4 (14 %) patients in group 2 had signs of lactose-dependent SIBO. According to HBT data, 21 (70 %) children in group 1 and 7 (25 %) persons in group 2 had lactose malabsorption. We also analyzed the data of glucose (Fig. 1) and lactose HBT (Fig. 2), depending on the presence of NAFLD and overweight/obesity. It was found that children with NAFLD had higher levels of hydrogen when conducting glucose and lactose HBT. Among children with NAFLD, lactose malabsorption was diagnosed in 17 (56.7 %) persons, lactose-dependent SIBO — in 15 (50.0 %). Ten (35.7 %) obese children without NAFLD had lactose malabsorption, and 9 (32.1 %) — lactose-dependent SIBO. Thus, in patients with NAFLD, lactose malabsorption was detected 1.6 times more often than in children without NAFLD.
Factors associated with SIBO in obese/overweight children
When analyzing risk factors associated with SIBO, following parameters were analyzed: NAFLD, abdominal obesity, hypertriglyceridemia, an increase in the HOMA, lactose malabsorption and lactose-dependent SIBO (Table 7).
/65-1.jpg)
It was found that children with NAFLD had 2-fold increased relative risk of developing SIBO.
Discussion
Our research has shown that obese/overweight children with SIBO were more likely to have NAFLD. Thus, SIBO was diagnosed in 70 % of patients with NAFLD, at the same time, 70 % of obese/overweight children with SIBO were diagnosed with NAFLD. According to literature sources, the prevalence of SIBO with NAFLD ranges from 50 to 77.8 % [3, 9, 20].
The composition of the intestinal microflora in subjects with obesity is represented by a smaller variety of intestinal bacteria, and altered by the expression of bacterial genes and metabolic pathways [7, 15]. Studies of microflora in patients with steatohepatitis suggest a lower content of Bacteroides/Prevotella than in those with simple steatosis, regardless of BMI and fat intake. Reducing Bacteroidetes may increase the overall energy consumption with food [10].
In our study, patients with SIBO were characterized by a higher level of ESR, indicating a relationship between this pathological condition and systemic inflammation. This can be explained by the fact that pathogen-associated molecular patterns of intestinal microorganisms penetrate through the portal vein system into the liver and are recognized by specific receptors, including TLR and NOD-like receptors. TLR binding to the corresponding ligands induces a powerful inflammatory cascade as a result of NF-kB activation, the production of proinflammatory cytokines, and the activation of JNK [8, 18].
The results of our research showed that patients with SIBO had higher hyperglycemic coefficient during OGTT, indicating a correlation between the intestinal microbiota and carbohydrate metabolism disorder. According to the literature, the activation of inflammatory pathways leads to an insult to insulin signaling, with a decrease in the phosphorylation of the insulin receptor, the insulin receptor substrate (IRS) and Akt, as well as suppressing serine phosphorylation of IRS-1 [7, 10]. The induction of metabolic endotoxemia in mice, by continuous subcutaneous infusion of lipopolysaccharides for four weeks, is accompanied by an increase in the following parameters: fasting glycemia, insulinemia, inflammatory markers, liver triglyceride content, insulin resistance [6].
The higher level of triglycerides and LDL in the group of children with SIBO can be explained by the high incidence of NAFLD among group 1 representatives. After all, NAFLD is characterized by the growth of TG and LDL. However, the direct effect of intestinal microbiota on lipid metabolism disorders in obese patients has been shown. In the distal part of the small intestine and colon, undigested carbohydrates, such as starch, dietary fiber and other poorly digestible polysaccharides, are fermented by saccharolytic bacteria that include Bacteroidetes, Firmicutes, and Actinobacteria with short-chain fatty acids. Short-chain fatty acids after absorption are a substrate for the synthesis of triglycerides in the liver and play an important role in the regulation of appetite, they can not only passively diffuse into circulation, but also act as signaling molecules [10, 19].
Another mechanism that explains the role of intestinal microflora in the pathogenesis of NAFLD is the change in the expression of genes involved in the de novo lipogenesis and inhibition of epithelial expression of the fasting-induced adipocyte factor (Fiaf), a suppressor of lipoprotein lipase. Fiaf is produced not only in the intestine, but also in the liver and adipose tissue, being an essential regulator of the accumulation of peripheral fat. By suppressing Fiaf, the microbiota enhances the activity of lipoprotein lipase in the adipose tissue, increasing the content of triglycerides, which determines the storage of TG in the liver [10, 16].
When conducting lactose HBT, the majority of children with NAFLD had a curve characterized by a rapid increase (within the first 60 minutes) in hydrogen concentration stored up to 90 minutes with a lack of decrease between the first and second highest rates. This may indicate a retrograde pass of the chyme to the small intestine through the ileocecal valve. Such situation in patients with lactose malabsorption is observed quite often, and is due to increased pressure in the intestine as a result of the process of fermentation of this disaccharide. According to Brazilian researchers, hypolactasia increases the risk of insulin resistance in patients with steatohepatitis [5]. According to the results of our work, majority of SIBO children had concomitant lactose malabsorption, which was found almost three times more often compared to obese/overweight children without SIBO. Also, the high frequency of lactose malabsorption in patients with NAFLD is noted compared to patients without NAFLD.
It is suggested that the use of milk and dairy products is associated with optimal insulin secretion, the absence of fluctuations in blood glucose level and increased secretion of glucagon-like peptide 1 and glucose-dependent insulinotropic polypeptide [5]. However, patients with hypolastasia do not have these benefits. A French cohort study, involving 3,575 patients, demonstrated that hypolactasia is associated with a higher incidence of glucose tolerance and type 2 diabetes mellitus [12]. Thus, on the one hand, the presence of lactose malabsorption in children with obesity can contribute to an increase in intraabdominal pressure with the further development of SIBO, and the presence of SIBO can lead to a disturbance in the lactose digestion. On the other hand, disorders of lactose digestion are associated with an adverse effect on carbohydrate metabolism, which aggravates the course of NAFLD.
It should be noted that in 14 % of children, who had a negative result of glucose HBT, lactose-dependent SIBO was detected, and 25 % had lactose malabsorption. These data suggest the need for a thorough history collection and examination of obesity patients with dyspeptic manifestations, as clinical data may often be attributed not only to SIBO, but also to lactose malabsorption and to lactose-dependent SIBO. After all, the SIBO in the studied patients had clinical manifestations as increased frequency of defecation, painful palpation in the hypogastrium.
To our knowledge, this is the first study on the evaluation of the state of small intestinal microbiota and carbohydrates digestion in NAFLD children using transient elastography. For the first time, the comparison of lactose and glucose HBT among obese/overweight children in general and among children with NAFLD in particular was provided. The limitation of work is the inability to exclude cases of H2-non-production, i.e., there was no control of methane level in the exhaled air for the purpose of diagnosing SIBO in H2-non-producers.
Conclusions
1. NAFLD in children can act as a risk factor for SIBO development.
2. SIBO is associated with signs of low-grade inflammation and adverse metabolic profile in the form of changes in lipid and carbohydrate metabolism, which may contribute to the development and progression of NAFLD.
3. Children with lactose malabsorption had three times higher relative risk of SIBO. At the same time, more than a half of NAFLD patients were characterized by the presence of lactose malabsorption and lactose-dependent SIBO according to lactose HBT.
4. Thus, timely diagnosis and correction of the existing disorders of the intestinal microflora, taking into account lactose digestion, is an important trend in preventing the progression of NAFLD in children.
Conflicts of interests. Authors declare the absence of any conflicts of interests and their own financial interest that might be construed to influence the results or interpretation of their manuscript.
1. Бабак О.Я., Лапшина К.А., Черняк А.М. Комплексне лікування неалкогольної жирової хвороби печінки: досвід застосування гепатопротекторів. Сучасна гастроентерологія. 2018. № 2(100). С. 32-36.
2. Наказ Міністерства охорони здоров’я України від 29.01.2013 № 59 «Про затвердження уніфікованих клінічних протоколів медичної допомоги дітям із захворюваннями органів травлення». Режим доступу: https://www.moz.gov.ua/ua/portal/dn_20090203_55.html
3. Belei O., Olariu L., Dobrescu A. et al. The relationship between non-alcoholic fatty liver disease and small intestinal bacterial overgrowth among overweight and obese children and adolescents. Journal of Pediatric Endocrinology and Metabolism. 2017. Vol. 30(11). P. 1161-1168. https://doi.org/10.1515/jpem-2017-0252.
4. Bush H., Clemente M.G., Mandato C. et al. Pediatric non-alcoholic fatty liver disease: Recent solutions, unresolved issues, and future research directions. World Journal of Gastroenterology. 2016. Vol. 22(36). P. 8078-8093. http://doi.org/10.3748/wjg.v22.i36.8078.
5. Campos Mazo D.F., Mattar R., Stefano J.T. et al. Hypolactasia is associated with insulin resistance in nonalcoholic steatohepatitis. World Journal of Hepatology. 2016. Vol. 8(24). P. 1019-1027. http://doi.org/10.4254/wjh.v8.i24.1019.
6. Cani Amar P.D., Iglesias M.A. Metabolic endotoxemia initiates obesity and insulin resistance. Diabetes. 2007. Vol. 56. P. 1761-1772. doi: 10.2337/db06-1491.
7. Caricilli A.M., Saad M.J. The role of gut microbiota on insulin resistance. Nutrients. 2013. Vol. 5. P. 829-851. doi: 10.3390/nu5030829.
8. Clemente M.G., Mandato C., Poeta M., Vajro P. Pediatric non-alcoholic fatty liver disease: Recent solutions, unresolved issues, and future research directions. World Journal of Gastroenterology. 2016. Vol. 22(36). P. 8078-8093. http://doi.org/10.3748/wjg.v22.i36.8078.
9. Fialho A., Fialho A., Thota P. et al. Small intestinal bacterial overgrowth is associated with non-alcoholic fatty liver disease. J. Gastrointestin. Liver Dis. 2016. Vol. 25(2). P. 159-65. doi: 10.15403/jgld.2014.1121.252.iwg.
10. Ferolla S.M., Armiliato G.N., Couto C.A., Ferrari T.C. The role of intestinal bacteria overgrowth in obesity-related nonalcoholic fatty liver disease. Nutrients. 2014. Vol. 6(12). P. 5583-5599. doi: 10.3390/nu6125583.
11. Gasbarrini A., Corazza G.R., Gasbarrini G. et al. Methodology and indications of H2-breath testing in gastrointestinal diseases: the Rome Consensus Conference. Alimentary Pharmacology & Therapeutics. 2009. Vol. 29. P. 1-49.
12. Lamri A., Poli A., Emery N. et al. The lactase persistence genotype is associated with body mass index and dairy consumption in the D.E.S.I.R. study. Metabolism. 2013. Vol. 62. P. 1323-1329.
13. Mercedes de Onis. World Health Organization Reference Curves. http://ebook.ecog-obesity.eu/chapter-growth-charts-body-composition/world-health-organization-reference-curves.
14. Nier A., Engstler A.J., Maier I.B., Bergheim I. Markers of intestinal permeability are already altered in early stages of non-alcoholic fatty liver disease: Studies in children. PLoS ONE. 2017. Vol. 12(9). P. e0183282. http://doi.org/10.1371/journal.pone.0183282.
15. Paolella G., Mandato C., Pierri L. et al. Gut-liver axis and probiotics: their role in non-alcoholic fatty liver disease. World J. Gastroenterol. 2014. Vol. 20(42). P. 15518-15531. doi: 10.3748/wjg.v20.i42.15518.
16. Perla F.M., Prelati M., Lavorato M. et al. The role of lipid and lipoprotein metabolism in non-alcoholic fatty liver disease. Children. 2017. Vol. 4(6). P. 46. http://doi.org/10.3390/children4060046.
17. Alberti G., Zimmet P., Kaufman F. et al. The IDF consensus definition of the metabolic syndrome in children and adolescents. International Diabetes Federation. 2007. P. 23.
18. Shanab A.A., Scully P., Crosbie O., Buckley M. et al. Small intestinal bacterial overgrowth in nonalcoholic steatohepatitis: association with toll-like receptor 4 expression and plasma levels of interleukin 8. Digestive Diseases and Sciences. 2011. Vol. 56(5). P. 1524-1534.
19. Troisi J., Pierri L., Landolfi A. et al. Urinary metabolomics in pediatric obesity and NAFLD identifies metabolic pathways/metabolites related to dietary habits and gut-liver axis perturbations. Nutrients. 2017. Vol. 9(5). P. 485. http://doi.org/10.3390/nu9050485.
20. Wigg A.J., Roberts-Thomson I.C., Dymock R.B. et al. The role of small intestinal bacterial overgrowth, intestinal permeability, endotoxaemia, and tumour necrosis factor alpha in the pathogenesis of non-alcoholic steatohepatitis. Gut. 2001. Vol. 48. P. 206-211.