Резюме
Актуальність. Дефекти кісток (ДК) — патологічний стан, що характеризується втратою об’єму кісткової тканини, який не може самостійно відновитись навіть за умови адекватних заходів та хірургічної стабілізації. У літературі такий стан характеризується як критичний дефект: довжина понад 2 см та втрата кісткової маси понад 50 %. ДК розподіляються на первинні або вторинні та є наслідком доволі широкого за своєю природою кола чинників: пухлини опорно-рухового апарату, інфекції, високоенергетичні пошкодження, остеофіброзні дисплазії або вроджені вади (Adams-Oliver syndrome). З початком повномасшабної агресії головним чинником як первинних, так і вторинних ДК стали бойові ураження (вогнепальні та мінно-вибухові), які виникають у результаті високоенергетичного комбінованого впливу та призводять до поліструктурних пошкоджень. Мета: порівняти клінічні результати методики Masquelet та методу транспортування кісток при лікуванні пацієнтів з сегментарними дефектами довгих кісток кінцівок. Матеріали та методи. У двох базах даних (PubMed, Embase) було проаналізовано сучасну літературу щодо лікування дефектів довгих трубчастих кісток за період з 2016 по 2025 р. з використанням методу Ілізарова — кістковий транспорт та Masquelet — індукована мембрана, за ключовими словами: bone defect, nonunion, bone transport, Masquelet method, complications. Результати. Найпоширенішими недоліками та ускладненнями при кістковому транспорті є довготривале використання зовнішньої конструкції, інфекція місця закріплення штифта (65,96 %), аксіальне відхилення (40,78 %), скутість суглоба (23,76 %), стискання м’яких тканин (22,34 %) та затримка зрощення місця стикування (13,48 %). Для зменшення їх кількості запропоновано цілу низку різнопланових удосконалень. Зокрема, набирає популярності трифокальний спосіб, застосування односторонніх зовнішніх фіксаторів з інтрамедулярними фіксаторами, інтрамедулярний кабельний транспорт, транспортування кістки за допомогою магнітних інтрамедулярних стрижнів. Позитивні результати при застосуванні методу Masquelet становлять близько 86 % проти 95 % при кістковому транспорті, однак перший демонструє переваги у нижчій вартості госпіталізації, коротшому часі остаточного зрощення до повного навантаження, нижчій частоті ускладнень та кращій післяопераційній якості життя. Висновки. Метод кісткового транспорту та Masquelet є сучасними найбільш вживаними технологіями при лікуванні пацієнтів з дефектами кісткової тканини. Позитивні результати при застосуванні цих методик становлять близько 86–95 %, що з урахуванням поліструктурних уражень є доволі значущим показником. Кожен метод характеризується своїми позитивними сторонами та недоліками, які зумовлені особливостями його реалізації та тяжкістю пошкодження, що потребує їх застосування за чітко визначеними показаннями.
Background. Bone defects are a pathological condition characterized by a loss of bone tissue volume that cannot be restored independently even with adequate measures and surgical stabilization. In the literature, this condition is described as a critical defect: length over 2 cm and bone mass loss over 50 %. Bone defects are divided into primary or secondary ones and are the result of a fairly wide range of factors: tumors of the musculoskeletal system, infections, high-energy injuries, osteofibrous dysplasias, or congenital defects (Adams-Oliver syndrome). With the beginning of full-scale aggression, combat injuries (fire and mine-explosive), which arise as a result of high-energy combined effects and lead to polystructural damage, became the main factor in both primary and secondary bone defects. Objective: to compare the clinical outcomes of using the Masquelet technique and bone transport in the treatment of patients with segmental defects of the long bones of the extremities. Materials and methods. In two databases (PubMed, Embase), the current literature was analyzed on the treatment of defects of long tubular bones from 2016 to 2025 with the help of the Ilizarov method (bone transport) and Masquelet technique (induced membrane) using the keywords: bone defect, nonunion, bone transport, Masquelet method, complications. Results. The most common disadvantages and complications of bone transport are long-term use of the external fixation device, infection of the pin site (65.96 %), axial deviation (40.78 %), joint stiffness (23.76 %), soft tissue compression (22.34 %), and delayed fusion of the junction (13.48 %). To reduce their number, various improvements have been proposed. In particular, the trifocal method, the use of unilateral external devices with intramedullary fixators, intramedullary cable transport, and bone transport using magnetic intramedullary rods are gaining popularity. Positive results when using the Masquelet method are about 86 versus 95 % with bone transport, but it demonstrates advantages in lower hospitalization costs, shorter time from final union to full load, lower complication rates, and better post-operative quality of life. Conclusions. Bone transport and Masquelet method are the most widely used modern techniques in the treatment of patients with bone defects. Positive results with the use of these techniques are about 86–95 %, which is quite significant considering polystructural lesions. Each method is characterized by advantages and disadvantages, which are determined by the specifics of its implementation and the severity of the injury, which requires the use according to clearly defined indications.
Список литературы
1. Tsang S.J., van Rensburg A.J., van Heerden J. еt аl. The management of critical bone defects: outcomes of a systematic approach. Eur J Orthop Surg Traumatol. 2024;34(6):3225-3231. doi: 10.1007/s00590-024-04050-1.
2. Грицай М., Колов Г., Сабадош В. та ін. Основні хірургічні методи заміщення критичних дефектів великогомілкової кістки (огляд літератури). Частина II. Tеrra orthopaedica. 2024;2(121):45-53. doi: 10.37647/2786-7595-2024-121-2-45-53.
3. Migliorini F., La Padula G., Torsiello E. et al. Strategies for large bone defect reconstruction after trauma, infections or tumour excision: a comprehensive review of the literature. Eur J Med Res. 2021;26:118. doi: 10.1186/s40001-021-00593-9.
4. Rashid S., Azeem S., Riaz S. Adams-Oliver Syndrome: A Rare Congenital Disorder. Cureus. 2022;14(3):23297. doi: 10.7759/cureus.23297.
5. Rupp M., Popp D., Alt V. Prevention of infection in open fractures: Where are the pendulums now? Injury. 2020;51(2):57-63. doi: 10.1016/j.injury.2019.10.074.
6. Altomare M., Granieri S., Cioffi S.P.B. et al. High-Grade Limbs Open Fractures: Time to Find Milestones in the Emergency Setting. Life (Basel). 2021;11(11):1226. doi: 10.3390/life11111226.
7. Benavides J.M., Benavides L.C., Pumiglia L. еt аl. Breaking point: Musculoskeletal combat injuries in Iraq, Afghanistan, and Syria-Epidemiology and future directions of care on the battlefield after over two decades of war. J Trauma Acute Care Surg. 2025;99(3):27-31. doi: 10.1097/TA.0000000000004705.
8. Prat D., Bloch A., Braun M. еt аl. Do Gunshot and Explosion Injuries Differ in Severity and Management? A Multicenter Study of Upper Extremity Trauma in the 2023 Israel-Gaza Conflict. Clin Orthop Relat Res. 2025. doi: 10.1097/CORR.0000000000003618.
9. Brown K.V., Roberts D.C., Wordsworth M. еt al. Ma–nagement of conflict injuries to the upper limb. Part 1: assessment and early surgical care. The Journal of Hand Surgery. 2022; European volume 47(7):687-697. https://doi.org/10.1177/17531934221098916.
10. Wild H., Stewart B.T., Le Boa C. еt al. Epidemiology of Injuries Sustained by Civilians and Local Combatants in Contemporary Armed Conflict: An Appeal for a Shared Trauma Re-gistry Among Humanitarian Actors. World Journal оf Surgery. 2020;44(6):1863-1873. doi: 10.1007/s00268-020-05428-y.
11. Burianov O., Yarmoliuk Yu., Derkach S. еt al. Criteria for predicting risks in the case of replacing an fixator with an internal fixator during the treatment of gunshot fractures of the extremities. Orthopaedics, Traumatology аnd Prosthtics. 2023;1:5-9. doi: 10.15674/0030-5987202315-9.
12. Murphy B., Irwin S., Condon F. The 50 most influential papers pertaining to the Ilizarov method: A bibliometric analysis. Journal of Оrthopaedics. 2022;30:30-35. doi: 10.1016/j.jor.2022.02.010.
13. Masquelet A.C., Giannoudis P.V. The induced membrane technique for treatment of bone defects: What have I learned? Trauma Case Reports. 2021;36:100556. doi: 10.1016/j.tcr.2021.100556.
14. Page M.J., McKenzie J.E., Bossuyt P.M. еt аl. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:71. doi: 10.1136/bmj.n71.
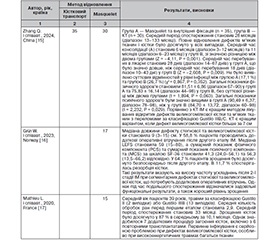
15. Kang Y., Wu Y., Ma Y., Jia X., Zhang M., Lin F., Rui Y. Masquelet combined with free-flap technique versus the Ilizarov bone transport technique for severe composite tibial and soft-tissue defects. Injury. 2024 Jun;55(6):111521. doi: 10.1016/j.injury.2024.111521.
16. Grn W., Hansen E.J.J., Andreassen G.S. еt аl. Functional outcomes and health-related quality of life after reconstruction of segmental bone loss in femur and tibia using the induced membrane technique. Arch Orthop Trauma Surg. 2023;143(8):4587-4596. doi: 10.1007/s00402-022-04714-9.
17. Mathieu L., Bilichtin E., Durand M. еt аl. Masquelet technique for open tibia fractures in a military setting. Eur J Trauma Emerg Surg. 2020;46(5):1099-1105. doi: 10.1007/s00068-019-01217-y.
18. Fung B., Hoit G., Schemitsch E. еt аl. The induced membrane technique for the management of long bone defects. Bone Joint J. 2020;102-B(12):1723-1734. doi: 10.1302/0301-620X.102B12.BJJ-2020-1125.R1.
19. Hsu C.A., Chen S.H., Chan S.Y. еt аl. The Induced Membrane Technique for the Management of Segmental Tibial Defect or Nonunion: A Systematic Review and Meta-Analysis. Biomed Res Int. 2020;2020:5893642. doi: 10.1155/2020/5893642.
20. Yoon Y.C., Kim Y., Song H.K. еt аl. Efficacy of Staged Surgery in the Treatment of Open Tibial Fractures with Severe Soft Tissue Injury and Bone Defect. Yonsei Med J. 2022;63(10):915-926. doi: 10.3349/ymj.2022.0078.
21. Chloros G.D., Kanakaris N.K., Harwood P.J. еt аl. Induced membrane technique for acute bone loss and nonunion management of the tibia. OTA Int. 2022;5(2):170. doi: 10.1097/OI9.0000000000000170.
22. Koodziejczyk K., Ropielewski A., Garlewicz R. еt аl. Clinical Observations of the Effectiveness of the Masquelet Induced Membrane Technique in the Treatment of Critical Long-Bone Defects of the Lower and Upper Extremities. Medicina (Kaunas). 2024;60(12):1933. doi: 10.3390/medicina60121933.
23. Tsang S.J., van Rensburg A.J., van Heerden J. еt аl. The management of critical bone defects: outcomes of a systematic approach. Eur J Orthop Surg Traumatol. 2024;34(6):3225-3231. doi: 10.1007/s00590-024-04050-1.
24. Shen J., Wei Z., Wang S. еt аl. Treatment of infected bone defects with the induced membrane technique. Bone Joint Res. 2023;12(9):546-558. doi: 10.1302/2046-3758.129.BJR-2022-0439.R2.
25. Wang P., Wu Y., Rui Y. еt аl. Masquelet technique for reconstructing bone defects in open lower limb fracture: Analysis of the relationship between bone defect and bone graft. Injury. 2021;52(4):988-995. doi: 10.1016/j.injury.2020.12.009.
26. zpolat N., Tunez M., Reisolu A. еt аl. Management of tibial non-unions with Masquelet technique after failed previous treatment options for Grade III open fractures. Ulus Travma Acil Cerrahi Derg. 2022;28(8):1180-1185. doi: 10.14744/tjtes.2021.36768.
27. Lu Y., Wang Q., Ren C. et al. Proximal versus distal bone transport for the management of large segmental tibial defect: a clinical case series. Sci Rep. 2023;13:3883. doi: 10.1038/s41598-023-31098-6.
28. Qian Wang, Teng Ma, Zhong Li et al. Bone transport combined with sequential nailing technique for the management of large segmental bone defects after trauma. Sec. Orthopedic Surgery. 2024;11. doi: 10.3389/fsurg.2024.1302325.
29. Liu Y., Yushan M., Liu Z. et al. Complications of bone transport technique using the Ilizarov method in the lower extremity: a retrospective analysis of 282 consecutive cases over 10 years. BMC Musculoskelet Disord. 2020;21:354. doi: 10.1186/s12891-020-03335-w.
30. Kinik H., Kalem M. Ilizarov segmental bone transport of infected tibial nonunions requiring extensive debridement with an average distraction length of 9,5 centimetres. Is it safe? Injury. 2021;52(8):2425-2433. doi: 10.1016/j.injury.2019.12.025.
31. Liu K., Jia Q., Wang X. et al. Complications associated with single-level bone transport for the treatment of tibial bone defects caused by fracture-related infection. BMC Musculoskelet Disord. 2023;24(1):514. doi: 10.1186/s12891-023-06527-2.
32. Xie J., Zhao G., Yasheng T. et al. Ilizarov bone transport to treat infected nonunion of long bones: a multicenter retrospective cohort study. J Int Med Res. 2021;49(3):3000605211002701. doi: 10.1177/03000605211002701.
33. Shi B., Zhang Z., Ji G. et al. Bone Transport for Large Segmental Tibial Defects Using Taylor Spatial Frame versus the Ilizarov Circular Fixator. Orthop Surg. 2024;16(9):2157-2166. doi: 10.1111/os.14192.
34. Huang Q., Ren C., Li M. et al. Antibiotic calcium sulfate-loaded hybrid transport versus traditional Ilizarov bone transport in the treatment of large tibial defects after trauma. J Orthop Surg Res. 2021;16(1):568. doi: 10.1186/s13018-021-02723-9.
35. Feng D., Zhang Y., Jia H. et al. Complications analysis of Ilizarov bone transport technique in the treatment of tibial bone defects — a retrospective study of 199 cases. BMC Musculoske–let Disord. 2023;24(1):864. doi: 10.1186/s12891-023-06955-0.
36. Yang X., Hamiti Y., Liu K. еt аl. Optimizing bone transport strategies: a pixel value ratio-based evaluation of rege-neration rates in bifocal and trifocal techniques. Front Surg. 2024;11:1494658. doi: 10.3389/fsurg.2024.1494658.
37. Hamiti Y., Abudureyimu P., Lyu G. еt аl. Trifocal versus Pentafocal bone transport in segmental tibial defects: a matched comparative analysis for posttraumatic osteomyelitis treatment. M.BMC Musculoskelet Disord. 2024;25(1):383. doi: 10.1186/s12891-024-07507-w. PMID: 38750523.
38. Xie L., Huang Y., Zhang L. еt аl. Ilizarov method and its combined methods in the treatment of long bone defects of the lower extremity: systematic review and meta-analysis. BMC Musculoskelet Disord. 2023;24(1):891. doi: 10.1186/s12891-023-07001-9.
39. Rosteius T., Ptzholz S., Rausch V. еt аl. Ilizarov bone transport using an intramedullary cable transportation system in the treatment of tibial bone defects. Injury. 2021;52(6):1606-1613. doi: 10.1016/j.injury.2020.12.028.
40. Summers S., Krkovic M. Bone transport with magnetic intramedullary nails in long bone defects. Eur J Orthop Surg Traumatol. 2021 Aug;31(6):1243-1252. doi: 10.1007/s00590-020-02854-5.
41. Alford A.I., Nicolaou D., Hake M. еt аl. Masquelet’s induced membrane technique: Review of current concepts and future directions. J Orthop Res. 2021;39(4):707-718. doi: 10.1002/jor.24978.
42. O’Connor C.M., Perloff E., Drinane J. еt аl. An Analysis of Complications and Bone Defect Length With the Use of Induced Membrane Technique in the Upper Limb: A Systematic Review. Hand (NY). 2022;17(3):572-577. doi: 10.1177/1558944720918368.
43. Pederiva D., De Luca L., Faldini C. еt аl. Masquelet’s induced membrane technique in the upper limb: a systematic review of the current outcomes. J Orthop Traumatol. 2025 Jan 27;26(1):4. doi: 10.1186/s10195-024-00815-w.
44. Ren C., Li M., Ma T. еt аl. A meta-analysis of the Masquelet technique and the Ilizarov bone transport method for the treatment of infected bone defects in the lower extremities. J Orthop Surg (Hong Kong). 2022;30(2):10225536221102685. doi: 10.1177/10225536221102685.