
Журнал «Травма» Том 26, №5, 2025
Вернуться к номеру
Прогнозування хронічного болю після тяжких ран за допомогою штучного інтелекту: пілотне відкрите дослідження
Авторы: A. Popelnukha, D. Dmytriiev
Vinnytsia National Pirogov Memorial Medical University, Vinnytsia, Ukraine
Center for the Treatment and Rehabilitation of Chronic Pain “Prometheus”, Vinnytsia, Ukraine
Рубрики: Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
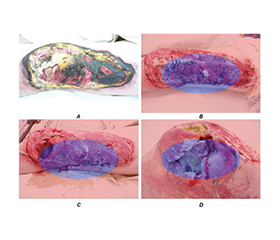
Актуальність. Тяжкі травматичні рани, особливо у військових умовах, часто ускладнюються розвитком хронічного, нейропатичного та фантомного болю. Раннє прогнозування больових синдромів залишається клінічною проблемою. Використання технологій штучного інтелекту (ШІ) відкриває нові можливості для інтеграції аналізу фотографій ран, мікробіологічних знахідок і даних щодо впливу медикаментів у прогностичні моделі. Мета: оцінити предиктори розвитку хронічного та нейропатичного болю після тяжких ран і перевірити точність платформи штучного інтелекту в прогнозуванні больових синдромів у військових. Матеріали та методи. Проспективне одноцентрове дослідження включало 311 військовослужбовців України з тяжкими ушкодженнями кінцівок (139 ампутацій). Збирали клінічні й демографічні дані, проводили мікробіологічні дослідження, аналізували серійні фото ран. У платформі використано штучний інтелект для сегментації ран, оцінки інфекції та прогнозування ризику розвитку хронічного, нейропатичного й фантомного болю. Результати аналізували через 3 і 6 місяців за шкалою NRS та опитувальником DN4. Результати. Через 6 місяців хронічний біль виявили у 42 % пацієнтів з ампутаціями, нейропатичний — у 29 %, фантомний — у 24 %. Незалежними предикторами були: інфекція рани (OR 2,1; 95% ДІ 1,4–3,2), затримка загоєння > 8 тижнів (OR 2,7; 95% ДІ 1,8–4,0), високий початковий рівень болю (NRS ≥ 7) (OR 1,9; 95% ДІ 1,2–3,0) і призначення нейротоксичних антибіотиків (OR 1,8; 95% ДІ 1,1–2,9). Платформа показала чутливість 78 %, специфічність 74 % та AUC 0,81. Висновки. Інфекція, затримка загоєння і прийом нейротоксичних препаратів є ключовими факторами ризику розвитку хронічного й нейропатичного болю після тяжких ран. Використання ШІ-платформи забезпечує клінічно значуще прогнозування ризику й може поліпшити персоналізоване лікування та реабілітацію військових.
Background. Severe traumatic wounds, particularly in military settings, are frequently complicated by chronic, neuropathic, and phantom limb pain. Early prediction of pain trajectories remains a clinical challenge. Advances in artificial intelligence (AI) enable integration of wound imaging, microbiology, and pharmacological data into predictive models. We developed and tested an AI-driven platform for the prediction of chronic and neuropathic pain after severe wounds. Materials and methods. A prospective observational study of 311 Ukrainian military patients with severe limb injuries (including 139 amputees) was conducted in 2022–2025. Clinical, demographic, and microbiological data were collected alongside serial wound photographs. The platform processed wound images to assess healing dynamics, identify infection-related risk, and compute the probability of chronic, neuropathic, and phantom pain. Pain outcomes were assessed at 3 and 6 months using the Numeric Rating Scale (NRS) and the DN4 questionnaire. Results. At 6 months, chronic pain was present in 42 % of patients, neuropathic pain in 29 %, and phantom pain in 24 % of amputees. Independent predictors of neuropathic pain included wound infection (odds ratio (OR) 2.1, 95% confidence interval (CI) 1.4–3.2), delayed wound healing (> 8 weeks) (OR 2.7, 95% CI 1.8–4.0), high baseline pain intensity (NRS ≥ 7) (OR 1.9, 95% CI 1.2–3.0), and exposure to neurotoxic antibiotics (OR 1.8, 95% CI 1.1–2.9). The platform achieved a sensitivity of 78 %, specificity of 74 %, and AUC of 0.81. Conclusions. Infection, delayed healing, and neurotoxic drug exposure are major predictors of chronic and neuropathic pain after severe wounds. The AI platform provides accurate, clinically relevant risk prediction and may support personalized pain prevention and rehabilitation in military trauma care.
хронічний біль; нейропатичний біль; фантомний біль; штучний інтелект; загоєння ран; військова травма; прогностична модель
chronic pain; neuropathic pain; phantom limb pain; artificial intelligence; wound healing; military trauma; prediction model