
Журнал «Боль. Суставы. Позвоночник» Том 15, №4, 2025
Вернуться к номеру
Мінеральна щільність кісткової тканини та маркери кісткового ремоделювання у військовослужбовців після ампутації нижніх кінцівок
Авторы: A.B. Vilenskyi (1), N.V. Grygorieva (2), O.Z. Stefiuk (3), I.I. Kaut (1), D.Yu. Kurylo (2), A.V. Iniushyna (2), T.Yu. Solonenko (2)
(1) - Superhumans Center, Lviv, Ukraine
(2) - D.F. Chebotarev Institute of Gerontology of the NAMS of Ukraine, Kyiv, Ukraine
(3) - Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
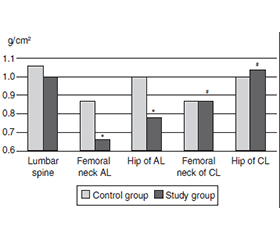
Актуальність. Війна в Україні зумовила зростання кількості ампутацій, які є частою причиною постіммобілізаційного остеопорозу. Мета: вивчити мінеральну щільність кісткової тканини (МЩКТ), статус вітаміну D і сироваткових маркерів кісткового ремоделювання у військовослужбовців-чоловіків з односторонньою ампутацією нижньої кінцівки внаслідок мінно-вибухових травм. Матеріали та методи. Обстежено 64 чоловіки віком 20–54 роки, поділених на 2 групи. Контрольну групу становили 32 здорові особи, дослідну — 32 чоловіки з трансфеморальною (ТФА) чи транстибіальною (ТТА) ампутацією. Середня тривалість постампутаційного періоду (ПАП) дорівнювала 5,0 [4,0–7,0] міс. МЩКТ оцінювали методом двохенергетичної рентгенівської денситометрії (Discovery Wi, Hologic), лабораторне дослідження включало вимірювання показників кальцій-фосфорного обміну, маркерів кісткового ремоделювання та рівня гідроксивітаміну D (25(ОН)D). Результати. МЩКТ проксимального відділу стегнової кістки та її шийки на стороні ампутації була вірогідно нижчою, ніж у контрольній групі (відповідно 0,78 ± 0,22 і 1,00 ± 0,20 г/см2; p = 0,0002, та 0,66 ± 0,20 і 0,87 ± 0,14 г/см2; p = 0,00002), проте вірогідних відмінностей у показниках МЩКТ контрлатеральної кінцівки порівняно зі здоровими особами не виявлено. Низьку МЩКТ проксимального відділу стегнової кістки чи її шийки (Z ≤ –2 SD) на стороні ампутації встановлено в 39–42 % пацієнтів дослідної групи без подібних змін контрлатерально та в контролі. Втрата МЩКТ ампутованої кінцівки становила ~ 20 % відносно контрлатеральної та зростала з тривалістю ПАП; при ТФА зниження МЩКТ було більш вираженим, ніж при ТТА. У 81 % пацієнтів з ампутаціями виявлено дефіцит/недостатність вітаміну D, а також вищий рівень P1NP порівняно зі здоровими особами. Уміст β-CTX був вірогідно вищим у пацієнтів із ТФА, ніж у представників контрольної групи. Висновки. У чоловіків з односторонніми травматичними ампутаціями нижньої кінцівки виявлено вірогідно нижчі показники МЩКТ на рівні ампутованої кінцівки порівняно зі здоровими особами. Втрата МЩКТ в ампутованій кінцівці при ТФА була вищою, ніж при ТТА, і збільшувалася з тривалістю ПАП. Значна частка чоловіків після ампутації нижньої кінцівки мали дефіцит/недостатність вітаміну D та вищі рівні P1NP порівняно з особами з контрольної групи. Отримані результати підкреслюють необхідність урахування стану кісткової тканини в цій категорії хворих у комплексних програмах реабілітації.
Background. The war in Ukraine has led to an increase in the number of amputations, which are a common cause of disuse osteoporosis. The purpose was to assess bone mineral density (BMD), vitamin D status, and serum bone turnover markers in war veterans with unilateral lower limb amputation resulting from mine-blast injuries. Materials and methods. A total of 64 men aged 20–54 years were examined and divided into two groups. The control group included 32 healthy subjects, while the study group consisted of 32 men with transfemoral (TFA) or transtibial (TTA) amputations (median post-amputation period (PAP): 5.0 [4.0–7.0] months). BMD was assessed using dual-energy X-ray absorptiometry (Discovery Wi, Hologic). Laboratory evaluation included parameters of calcium-phosphorus metabolism, bone remodeling markers, and serum 25-hydroxyvitamin D (25(OH)D). Results. BMD of the hip and femoral neck on the amputated side was significantly lower compared to controls (0.78 ± 0.22 vs. 1.00 ± 0.20 g/cm2; p = 0.0002 and 0.66 ± 0.20 vs. 0.87 ± 0.14 g/cm2; p = 0.00002, respectively). However, no significant differences were found for the contralateral limb compared to controls. Low BMD (Z ≤ –2 SD) on the amputated side was detected in 39–42 % of the persons from the study group, but not in contralateral limbs or controls. Bone loss in the amputated limb was ~ 20 % compared to the contralateral side, increasing with PAP duration, and was more pronounced in TFA than TTA. Vitamin D deficiency/insufficiency was found in 81 % of amputees, and higher P1NP level was found compared to controls. β-CTX level wase significantly higher in TFA group compared with controls. Conclusions. Men with traumatic unilateral lower limb amputations demonstrated significantly lower BMD in the amputated but not contralateral limb compared to controls. Bone loss was greater in TFA versus TTA and increased with PAP duration. A large proportion of amputees exhibited vitamin D deficiency/insufficiency and elevated serum P1NP level. These findings highlight the need to consider bone health in comprehensive rehabilitation programs for this patient group.
ампутація; нижня кінцівка; бойова травма; мінеральна щільність кісткової тканини; 25(ОН)D; маркери кісткового обміну; остеопороз
amputation; lower limb; combat; bone mineral density; 25(OH)D; bone turnover markers; osteoporosis
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Esfandiari E, Yavari A, Karimi A, Masoumi M, Soroush M, Saeedi H. Long-term symptoms and function after war-related lower limb amputation: a national cross-sectio–nal study. Acta Orthop Traumatol Turc. 2018;52(5):348-351. doi: 10.1016/j.aott.2017.04.004.
- Chopra A, Azarbal AF, Jung E, et al. Ambulation and functional outcome after major lower extremity amputation. J Vasc Surg. 2018;67(5):1521-1529. doi: 10.1016/j.jvs.2017.10.051.
- Rolvien T, Amling M. Disuse osteoporosis: clinical and mechanistic insights. Calcif Tissue Int. 2022;110(5):592-604. doi: 10.1007/s00223-021-00836-1.
- Grygorieva N, Dedukh N, Parubets M, Bystrytska M. Disuse (post-mobilization) osteoporosis: literature review and clinical case series. Pain Joints Spine. 2022;12(3):94-107. doi: 10.22141/pjs.12.3.2022.335 (in Ukrainian).
- Man J, Graham T, Squires-Donelly G, Laslett AL. The effects of microgravity on bone structure and function. NPJ Microgravity. 2022;8(1):9. doi: 10.1038/s41526-022-00194-8.
- Coulombe JC, Senwar B, Ferguson VL. Spaceflight-induced bone tissue changes that affect bone quality and increase fracture risk. Curr Osteoporos Rep. 2020;18(1):1-12. doi: 10.1007/s11914-019-00540-y.
- Bloomfield SA. Changes in musculoskeletal structure and function with prolonged bed rest. Med Sci Sports Exerc. 1997;29(2):197-206. doi: 10.1097/00005768-199702000-00006.
- Zheng X, Qi Y, Zhou H, Kang H, Tong Y, Bi L. Bone mineral density at the distal femur and proximal tibia and related factors during the first year of spinal cord injury. Int J Gen Med. 2021;14:1121-1129. doi: 10.2147/ijgm.s297660.
- Saleh I, Akbar A, Hasan HS, Yulisa ND, Aprilya D. Clinical characteristics and bone mineral density score in post-stroke neuromuscular deficit. J Clin Med Res. 2025;17(2):119-124. doi: 10.14740/jocmr6070.
- Luan H, Gu H, Mo Z, et al. The bone alterations in hind limb amputation rats in vivo. Med Nov Technol Devi–ces. 2020;8:100046. doi: 10.1016/j.medntd.2020.100046.
- Sherk VD, Bemben MG, Bemben DA. BMD and bone geometry in transtibial and transfemoral amputees. J Bone Miner Res. 2008;23(9):1449-1457. doi: 10.1359/jbmr.080402.
- Bemben DA, Sherk VD, Ertl WJJ, Bemben MG. Acute bone changes after lower limb amputation resulting from traumatic injury. Osteoporos Int. 2017;28(7):2177-2186. doi: 10.1007/s00198-017-4018-z.
- Smith É, Comiskey C, Carroll Á, Ryall N. A study of bone mineral density in lower limb amputees at a national prosthetics center. J Prosthet Orthot. 2011;23(1):14-20. doi: 10.1097/jpo.0b013e318206dd72.
- Finco MG, Kim S, Ngo W, Menegaz RA. A review of musculoskeletal adaptations in subjects following major lower-limb amputation. J Musculoskelet Neuronal Interact. 2022;22(2):269-283.
- McMenemy L, Behan FP, Kaufmann J, et al. Association between combat-related traumatic injury and skeletal health: bone mineral density loss is localized and correlates with altered loading in amputees: the Armed Services Trauma Rehabilitation Outcome (ADVANCE) Study. J Bone Miner Res. 2023;38(9):1227-1233. doi: 10.1002/jbmr.4794.
- Flint JH, Wade AM, Stocker DJ, Pasquina PF, Ho–ward RS, Potter BK. Bone mineral density loss after combat-related lower extremity amputation. J Orthop Trauma. 2014;28(4):238-244. doi: 10.1097/bot.0b013e3182a66a8a.
- Osterkamp LK. Current perspective on assessment of human body proportions of relevance to amputees. J Am Diet Assoc. 1995;95(2):215-218. doi: 10.1016/s0002-8223(95)00050-x.
- ISCD Official Positions 2023. Available from: https://iscd.org/official-positions-2023.
- Pludowski P, Takacs I, Boyanov M, et al. Clinical practice in the prevention, diagnosis and treatment of vitamin D deficiency: a Central and Eastern European expert consensus statement. Nutrients. 2022;14(7):1483. doi: 10.3390/nu14071483.
- Grygorieva N, Tronko M, Kovalenko V, et al. Diagnosis, prevention and treatment of vitamin D deficiency in adults: Ukrainian experts consensus statement. Pain Joints Spine. 2023;13(2):60-76. doi: 10.22141/pjs.13.2.2023.368 (in Ukrainian).
- Edwards DS, Phillip RD, Bosanquet N, Bull AM, Clasper JC. What is the magnitude and long-term economic cost of care of the British military Afghanistan amputee cohort? Clin Orthop Relat Res. 2015;473(9):2848-2855. doi: 10.1007/s11999-015-4250-9.
- Dougherty PJ, McFarland LV, Smith DG, Reiber GE. Bilateral transfemoral/transtibial amputations due to battle injuries: a comparison of Vietnam veterans with Iraq and Afghanistan service members. Clin Orthop Relat Res. 2014;472(10):3010-3016. doi: 10.1007/s11999-014-3534-9.
- Jin S, An CH, Jeong HY, et al. Importance of bilateral hip assessments in unilateral lower-limb amputees: a retrospective review involving older veterans. J Clin Med. 2024;13(14):4033. doi: 10.3390/jcm13144033.
- Buettmann EG, Goldscheitter GM, Hoppock GA, Friedman MA, Suva LJ, Donahue HJ. Similarities between disuse and age-induced bone loss. J Bone Miner Res. 2022;37(8):1417-1434. doi: 10.1002/jbmr.4643.
- Kulkarni J, Adams J, Thomas E, Silman A. Association between amputation, arthritis and osteopenia in British male war veterans with major lower limb amputations. Clin Rehabil. 1998;12(4):348-353. doi: 10.1191/026921598672393611.
- Cho H, Park J, Kim B, Han K, Choi HL, Shin DW. Increased risk of fracture after traumatic amputation: a nationwide retrospective cohort study. Healthcare (Basel). 2024;12(13):1362. doi: 10.3390/healthcare12131362.
- Haleem S, Yousaf S, Hamid T, Nagappa S, Par–ker MJ. Characteristics and outcomes of hip fractures in lower limb amputees. Injury. 2021;52(4):914-917. doi: 10.1016/j.injury.2020.10.017.
- Denton JR, McClelland SJ. Stump fractures in lower extremity amputees. J Trauma. 1985;25(11):1074-1078.
- Hunter SW, Batchelor F, Hill KD, et al. Risk factors for falls in people with a lower limb amputation: a systematic review. PMR. 2017;9:170-180. doi: 10.1016/j.pmrj.2016.07.531.
- Steinberg N, Gottlieb A, Siev-Ner I, Plotnik M. Fall incidence and associated risk factors among people with a lower limb amputation during various stages of recovery: a systematic review. Disabil Rehabil. 2019;41(15):1778-1787. doi: 10.1080/09638288.2018.1449258.
- Grygorieva N, Solonenko T, Musiienko A. Vitamin D deficiency during the COVID-19 pandemic and war in Ukraine. Pain Joints Spine. 2023;13(1):7-14. doi: 10.22141/pjs.13.1.2023.352 (in Ukrainian).
- Povoroznyuk V, Pankiv I, Zaverukha N, Solonenko T, Musiienko A. Levels of bone turnover markers (N-terminal propeptide of type I procollagen and carboxy-terminal telopeptide of type I collagen) in Ukrainian population of different age and gender. Int J Endocrinol (Ukraine). 2020;16(7):515-525. doi: 10.22141/2224-0721.16.7.2020.219005 (in Ukrainian).