
Архив офтальмологии Украины Том 11, №3, 2023
Вернуться к номеру
Фактори ризику розвитку оклюзій артерій сітківки після кардіохірургічних втручань при клапанних вадах серця
Авторы: Панченко Ю.О., Ковальчук Н.Я.
Національний університет охорони здоров’я України імені П.Л. Шупика, м. Київ, Україна
ДУ «Інститут серця» МОЗ України, м. Київ, Україна
Рубрики: Офтальмология
Разделы: Клинические исследования
Версия для печати
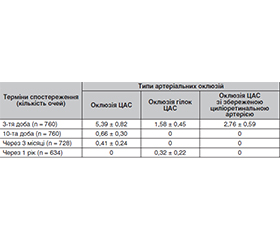
Актуальність. Є повідомлення про розвиток оклюзії центральної артерії сітківки (ОЦАС) після інвазивних серцево-судинних процедур. Хірургічне втручання, операція на відкритому серці та післяопераційна кровотеча підвищували ризик ОЦАС. У кардіохірургії виокремлюють певні фактори ризику для ОЦАС, як-от: гігантоклітинний артеріїт, каротидний стеноз, інсульт, стан гіперкоагуляції, цукровий діабет з офтальмологічними ускладненнями, гострий коронарний синдром, фібриляція передсердь, застійна серцева недостатність, а також куріння. Матеріали та методи. Під спостереженням перебувало 380 пацієнтів (760 очей) із клапанною патологією серця після кардіохірургічних втручань. Проводилося дослідження характеру, частоти й особливостей розвитку та клінічного перебігу оклюзій артерій сітківки у цих хворих. Для виявлення факторів ризику розвитку оклюзій артерій сітківки у пацієнтів із клапанними вадами серця після кардіохірургічних операцій була вивчена залежність їх частоти від статі, віку, виду оперативного втручання, типу протеза серцевого клапана й операційного доступу. Результати. Частота артеріальних оклюзій сітківки після проведених кардіохірургічних втручань протягом 1 року спостережень у середньому становила 11,12 % (χ2 = 173,645; p < 0,001). При аналізі типів артеріальних оклюзій зафіксовано розвиток усіх типів оклюзій на 3-тю добу. На 10-ту добу та через 3 місяці спостерігалася тільки оклюзія ЦАС — 0,66 і 0,41 % відповідно. Через 1 рік було діагностовано тільки оклюзію гілки ЦАС — 0,32 %. Частота артеріальних оклюзій вища втричі у пацієнтів з віковим проміжком від 51 до 70 років і вдвічі у пацієнтів віком понад 71 рік порівняно з пацієнтами вікового діапазону 50 років і молодше (p = 0,042); після протезування клапанів частота оклюзій удвічі вища (p = 0,034), ніж після пластики; при використанні механічних імплантів частота оклюзій артерій сітківки збільшується на 62 % (p = 0,010) порівняно з біологічними імплантами; при використанні класичного доступу під час операції частота оклюзій артерій сітківки статистично значуще вища на 35 % порівняно з мінідоступом та в 11 разів порівняно з доступом через стегнову артерію (р < 0,001).
Background. There are reports on the development of central retinal artery occlusion (CRAO) after invasive cardiovascular procedures. Surgery, open heart surgery, and postoperative bleeding increased the risk of CRAO. Cardiac surgery identifies certain risk factors for CRAO such as giant cell arteritis, carotid stenosis, stroke, hypercoagulable state, diabetes with ophthalmic complications, acute coronary syndrome, atrial fibrillation, congestive heart failure, and smoking. Materials and methods. Three hundred and eighty patients (760 eyes) with valvular heart disease after cardiosurgical interventions were under observation. A study on the nature, frequency and features of the occurrence and clinical course of retinal artery occlusions was conducted. To identify risk factors for the development of retinal artery occlusions in patients with valvular heart disease after cardiac surgery, the dependence of their frequency on gender, age, type of operation, type of heart valve prosthesis and surgical access was studied. Results. The frequency of retinal arterial occlusions after cardiosurgical interventions during 1 year of observation averaged 11.12 % (χ2 = 173.645; p < 0.001). When analyzing the types of arterial occlusions, the development of all types of occlusions was recorded on the 3rd day. On the 10th day and after 3 months, there was only CRAO, 0.66 and 0.41 %, respectively. After 1 year, only occlusion of the central retinal artery branch was diagnosed (0.32 %). The frequency of arterial occlusions is 3 times higher in patients aged 51 to 70 years and 2 times higher in those older than 71 years than in participants aged under 50 years (p = 0.042). After valve replacement, the frequency of occlusions is 2 times higher (p = 0.034) than after valvuloplasty. When using mechanical implants, the frequency of retinal artery occlusions increases by 62 % (p = 0.010) compared to biological implants. If classical access is used during surgery, the frequency of retinal artery occlusions is statistically significantly higher, by 35 % compared to mini access and by 11 times compared to femoral artery access (p < 0.001).
оклюзія центральної артерії сітківки; оклюзія гілки центральної артерії сітківки; клапанні вади серця; кардіохірургічне втручання
central retinal artery occlusion; occlusion of a branch of the central retinal artery; valvular heart defects; cardiosurgical intervention
Для ознакомления с полным содержанием статьи необходимо оформить подписку на журнал.
- Dattilo M., Newman N.J., Biousse V. Acute retinal arterial ischemia. Ann. Eye Sci. 2018 Jun. 3. 28. doi: 10.21037/aes.2018.05.04. Epub 2018 Jun 6. PMID: 30198015; PMCID: PMC6124502.
- Abdellah M.M. Multimodal Imaging of Acute Central Retinal Artery Occlusion. Med. Hypothesis Discov. Innov. Ophthalmol. 2019 Winter. 8(4). 283-290. Epub 2019 Oct 1. PMID: 31788490; PMCID: PMC6778676.
- Cho S.C., Jung C., Lee J.Y., Kim S.J., Park K.H., Woo S.J. Retinal Artery Occlusion аfter Intravascular Procedures: Case Series and Literature Review. Retina. 2019 Apr. 39(4). 766-778. doi: 10.1097/IAE.0000000000002008. PMID: 29266046.
- Arnold A.C. Urgent evaluation of the patient with acute central retinal artery occlusion. Am. J. Ophthalmol. 2018. 196. xvi-xvii. doi: 10.1016/j.ajo.2018.08.033.
- Hayreh S.S. Ocular vascular occlusive disorders: natural history of visual outcome. Prog. Retin. Eye Res. 2014 Jul. 41. 1-25.
- Monés J., Srivastava S.K., Jaffe G.J., Tadayoni R., Albini T.A., Kaiser P.K., et al. Risk of Inflammation, Retinal Vasculitis, and Retinal Occlusion-Related Events with Brolucizumab: Post Hoc Review of HAWK and HARRIER. Ophthalmology. 2021 Jul. 128(7). 1050-1059.
- Kapoor K.M., Kapoor P., Heydenrych I., Bertossi D. Vision loss associated with hyaluronic acid fillers: a systematic review of literature. Aesthetic Plast. Surg. 2020. 44. 929-944.
- Vadana M., Cecoltan S., Ciortan L., Macarie R.D., Tucureanu M.M., Mihaila A.C., et al. Molecular mechanisms involved in high glucose-induced valve calcification in a 3D valve model with human valvular cells. J. Cell. Mol. Med. 2020 Jun. 24(11). 6350-6361.
- Yen J.C., Lin H.L., Hsu C.A., Li Y.C., Hsu M.H. Atrial Fibrillation and Coronary Artery Disease as Risk Factors of Retinal Artery Occlusion: A Nationwide Population-Based Study. Biomed Res. Int. 2015. 2015. 374616.
- Hsien Y.M., Mustapha M., Hamzah J.C., Maskon O., Ken C.C., Hamdi C.H. Why can’t I see after my heart is fixed: a case series of ocular complications after cardiac intervention. BMC Ophthalmol. 2016 Mar 25. 16. 32.
- Grover V., Jangra K. Perioperative vision loss: A complication to watch out. J. Anaesthesiol. Clin. Pharmacol. 2012. 28(1). 11-6.
- Nenekidis I. et al. Vision impairment during cardiac surgery and extracorporeal circulation: current understanding and the need for further investigation. Acta Ophthalmol. 2012. 90(3). 168-72.