Introduction
Gastrointestinal cancer is one of the most common causes of death from neoplasms in European countries, and more than 3.4 million people die from it every year in the world [1]. Non-standard extended and combined interventions on several organs using the latest technologies and performing cytoreduction have become everyday surgical practice [2].
Although international guidelines recommend multiorgan resections for advanced colorectal cancer, morbidity and mortality rates associated with these complex interventions limit the number of patients who receive this treatment according to literature data [3]. The presence of positive resection margins, lymph node metastases and postoperative complications negatively affected the survival [3, 4]. Multiorgan resections are performed to treat patients with T4 cancer as the only option to achieve therapeutic resection, although the long-term survival of these patients remains low [2, 5].
The study of the state of oxidative modification of proteins, the restoration of indicators of the enzymatic state and lipid peroxidation in oncology has been conducted in many clinics around the world for several decades now, which gives us the advantage in determining the correlation between the disturbance of the redox imbalance and its further deterioration in cancer [6]. According to literature data, the activity of redox metabolism and markers of systemic chronic inflammation increases during the formation of oxidative stress [7, 8]. Therefore, their laboratory control is feasible in all conditions involving intoxication and the development of stress in the body, especially during multiorgan resections in cancer patients. It is very important to study the correction of disorders when using various options in their perioperative therapy [9]. In our study, the use of L-ornithine L-aspartate with quercetin was the most interesting.
A modern solution to this problem is the control of protein disorders against the background of correction of protein oxidation by means of a complex effect on all links of the repair process [10]. Of course, it is interesting to study the improvement of redox metabolism [11] and markers of systemic chronic inflammation, provided that the intensive care described by us is used to further reduce the incidence of complications and mortality (which we evaluated in terms of overall survival [12]). The biological meaning of our intensive care is to break the mechanism of the harmful effects of protein metabolites, control the enzymatic state and lipid peroxidation, improve reparative processes and inhibit the triggering of the apoptosis mechanism [13].
Purpose. Correction of redox metabolism based on the data of the oxidative modification of proteins, degree of their catabolic reaction, and data on the enzymatic state and lipid peroxidation in cancer patients with multiorgan resections on the gastrointestinal tract under conditions of perioperative intensive care.
Materials and methods
The study examined 117 cancer patients aged 67.6 ± 3.7 years with locally advanced tumor process of the gastrointestinal tract who underwent surgical interventions with multiorgan resections for health reasons. They were divided into two groups: I — controls (n1 = 55) in which antioxidant agents were not previously used; group II (n2 = 62) in which L-ornithine L-aspartate antioxidant protection was used (5 mg/10 ml, 10 ml twice a day intravenously, 500 ml saline) with a combination of quercetin and povidone (lyophilisate for solution of 0.5 g twice a day intravenously per 100 ml of saline). Intensive care was conducted in the form of antioxidant therapy for two days before surgery, intraoperatively and for three days in the postoperative period.
Studies were conducted preoperatively, on the 4th day and the 2nd week of the postoperative period. All patients were comparable in terms of their clinical characteristics, and all norms during research were observed in accordance with the standards of biomedical research and international ethical standards in science.
To determine the oxidative modification of proteins, serum biochemical measurements were performed. To assess the oxidative modification of proteins, the method of A.Z. Reznick and L. Parker modified by E.E. Dubinina was used, based on the interaction of amino acid derivatives with 2,4-dinitrophenylhydrazine and the formation of dinitrophenylhydrazones. Next, to assess fragmentation, acid-soluble peptides in the ultraviolet region at wavelengths of 254 nm (fine), 270 nm (medium) and 280 nm (large) in spontaneous (S254, S270, S280, respectively) and induced reactions (I254, I270, I280, respectively) were determined spectrophotometrically in the supernatant. The degree of oxidative modification of proteins was expressed in units of optical density per 1 mg of protein.
The method for assessing the oxidative modification of proteins in conjunction with the level of medium-weight molecules can be used in accordance with the reaction with 2,4-dinitrophenylhydrazine to form aldehyde and carbonyl derivatives of proteins (2,4-dinitrophenylhydrazones). The study of the oxidative modification of proteins was carried out on a spectrophotometer SF-46 at four wavelengths: at 356 nm, neutral aliphatic aldehyde dinitrophenylhydrazones were registered, at 370 nm — neutral aliphatic ketone-dinitrophenylhydrazones, at 430 and 530 nm — alkaline aliphatic aldehyde dinitrophenylhydrazones and ketone dinitrophenylhydrazones.
Biochemical measurements of indicators of the enzymatic state and lipid peroxidation were performed according to the content of superoxide dismutase, catalase, glutathione peroxidase in erythrocytes and α-tocopherol acetate in the serum of patients and were evaluated spectrophotometrically.
The serum content of malondialdehyde was determined spectrophotometrically at λ = 532 nm using the method of I.D. Stalnaya and T.G. Garishvili by reaction with thiobarbituric acid to form a trimethyl complex. The plasma level of nitrite-dependent metabolites is measured spectrophotometrically at λ = 540 nm with Griess reagent.
The levels of circulating tumor necrosis factor alpha (TNF-α), interleukin (IL) 6 and 8 in the serum were determined using enzyme immunoassay tests.
A preliminary assessment of the nature of the distribution of indicators was carried out by a visual method and the Shapiro-Wilk test. Statistical processing of the results was performed using the Statistica 10 software package, with the Student’s t-test and the Mann-Whitney U test. For each sample, the median (Me) was determined, and the upper and lower quartiles [Q1; Q3].
For the analysis of survival, statistical methods (construction of survival curves using the Kaplan-Meier method, estimation of the median survival) and log-rank test (for comparing survival curves) were used. Four hours after surgery was considered the beginning of the observation, which lasted 3 years. The end-point was combined and was defined as the time until death. In order to search for predictors of survival, a univariate analysis was applied using Cox regression followed by estimating the Exp(B) (hazard ratios) and 95% confidence interval (CI). For quantitative variables, with the purpose of comparative analysis of survival curves, division into groups was performed using the median.
Differences were considered statistically significant at p < 0.05 or tend to be significant at 0.1 > p > 0.05.
Results
Table 1 shows the studies of the oxidative modification of proteins at the stages of perioperative intensive care in cancer patients with multiorgan resections.
As can be seen from Table 1, in the control group the indicators for neutral aldehyde products (absorption maximum at 356 nm) changed from 0.048 ± 0.003 to 0.039 ± 0.001 and 0.042 ± 0.001, p < 0.05; for neutral ketone products (absorption maximum at 370 nm) — from 0.052 ± 0.003 to 0.043 ± 0.002 and 0.040 ± 0.003; for alkaline aldehyde products (absorption maximum at 430 nm) — from 0.030 ± 0.003 to 0.023 ± 0.003 and 0.020 ± 0.003, p < 0.05; for alkaline ketone products (absorption maximum at 530 nm) — from 0.028 ± 0.001 to 0.015 ± 0.003 and 0.011 ± 0.002, respectively, on the 4th day and 2nd week of the postoperative period.
/86.jpg)
Indicators for products of oxidative modification of proteins in spontaneous reactions at a wavelength of 254 nm (S254) changed from 1.854 ± 0.021 to 1.799 ± 0.017 and 1.711 ± 0.031; for S270 — from 0.236 ± 0.014 to 0.238 ± 0.005 and 0.248 ± 0.004; for S280 — from 0.134 ± 0.004 to 0.114 ± 0.001 and 0.104 ± 0.003. In iron-induced reactions for I254, they changed from 2.238 ± 0.016 to 2.211 ± 0.012 and 2.201 ± 0.011; for I270 — from 0.418 ± 0.017 to 0.391 ± 0.012 and 0.376 ± 0.007; for I280 — from 0.322 ± 0.012 to 0.303 ± 0.007 and 0.319 ± 0.004.
In the group with antioxidant protection, the indices for neutral aldehyde products (at a wavelength of 356 nm) changed from 0.051 ± 0.002 to 0.041 ± 0.002 and 0.039 ± 0.003, p < 0.05; for neutral ketone products (absorption maximum at 370 nm) — from 0.049 ± 0.003 to 0.041 ± 0.003 and 0.032 ± 0.001; for the alkaline aldehyde products (absorption maximum at 430 nm) — from 0.028 ± 0.002 to 0.019 ± 0.003 and 0.015 ± 0.002, р < 0.05; for the alkaline ketone products (at a wavelength of 530 nm) — from 0.019 ± 0.003 to 0.009 ± 0.003 and 0.008 ± 0.003.
When conducting intensive care, the indicators for products of oxidative modification of proteins were as follows: for S254 — changed from 1.863 ± 0.022 to 1.757 ± 0.020 and 1.701 ± 0.022; for S270 — from 0.234 ± 0.014 to 0.199 ± 0.009 and 0.212 ± 0.010; for S280 — from 0.131 ± 0.003 to 0.112 ± 0.002 and 0.103 ± 0.001.
In iron-induced reactions, the indicators for I254 changed from 2.225 ± 0.032 to 1.998 ± 0.018 and 1.755 ± 0.022; for I270 — from 0.392 ± 0.013 to 0.309 ± 0.017 and 0.283 ± 0.009; for I280 — from 0.319 ± 0.003 to 0.267 ± 0.004 and 0.251 ± 0.011.
Table 2 shows the studies of enzymes of the antioxidant system and lipid peroxidation metabolites at the stages of perioperative intensive care in cancer patients during multiorgan resections.
The study of antioxidant enzymes in the preoperative period in patients with multiorgan surgical interventions showed that in the control group the values of superoxide dismutase, glutathione peroxidase, α-tocopherol acetate did not differ significantly, but the level of catalase in the group receiving antioxidant therapy was somewhat higher (6.72 ± 0.10 units/min/g versus 9.86 ± 0.93 units/min/g, р < 0.05).
Changes in the content of lipid peroxidation products of cell membranes in the control group were significant but to a small extent. On the 4th day and the 2nd week of the postoperative period compared to the preoperative period, the level of malondialdehyde slightly decreased, and the content of nitrite-dependent metabolites increased slightly.
During the three-year follow-up of 117 patients with multiorgan resections, 12 (10.26 %) died, 2 (16.67 %) of them received antioxidant protection.
The levels of TNF-α, IL-6 and IL-8 turned out to be indicators that determine the survival of patients with multiorgan resections (Table 3).
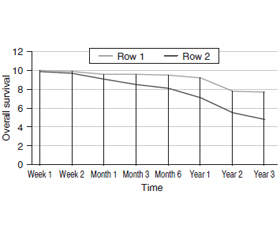
The median survival in the group of patients with the level of TNF-α < 26.37 pg/ml was 8.7 months, and in the group of patients with the level of TNF-α > 26.37 pg/ml — 5.9 months. Difference between groups by log-rank test was reliable, p = 0.037 (Fig. 1).
The median survival in the group of patients with the level of IL-6 < 31.11 pg/ml was 11.8 months, and in those with the level of IL-6 > 31.11 pg/ml — 5.7 months. Difference between groups by log-rank test was reliable, p = 0.039 (Fig. 2).
The median survival in the group of patients with the level of IL-8 < 13.42 pg/ml was 10.8 months, and in the group with the level of IL-8 > 13.42 pg/ml — 4.9 months. Difference between groups by log-rank test was reliable, p = 0.041 (Fig. 3).
Discussion
According to researchers, in oxidative stress, reactive oxygen species cause damage to all human cells. This leads to denaturation and defragmentation of proteins with excessive oxidative modification of proteins. Formed ionized amino acid fragments react with neighboring amino acids causing impaired protein metabolism and also reparative processes. According to the literature, indicators of oxidative modification of proteins are early signs of damage to tissues and organs, which gives us every reason to talk about the need for continuous laboratory monitoring of its processes in routine practice [14].
The study of the oxidative modification of proteins at the stages of perioperative intensive care in patients with multiorgan resections showed that the indicators in the control group on the 4th day of the postoperative period were significantly reduced compared to the preoperative period, and later, on the 2nd week of the postoperative period, they further decrease.
In the group of antioxidant protection, the indices more reliably decreased on the 4th day of the postoperative period, and later, on the 2nd week.
We also see that under the influence of intensive care, there was a more reliable reduction of modified proteins. At the same time, the indicators in the control group decreased slightly, and these changes were transient.
Subsequently, as seen from Table 2, in the group that received antioxidant protection, the indicators of enzymatic support increased more clearly on the 4th day and the 2nd week of the postoperative period, and the metabolites of lipid peroxidation decreased.
The data we have on the content of antioxidant enzymes and lipid peroxidation metabolites at the stages of intensive care of patients with multiorgan resections in the control group indicate an insufficient enzymatic maintenance of the redox balance on the 4th day and the 2nd week of the postoperative period. When antioxidant intensive care was carried out, the activity of antioxidant enzymes significantly increased, the metabolites of lipid peroxidation decreased, which can be explained by the influence of the means used and by the activation of the adaptation reserves of the body. It should be noted that the positive effect of our therapy persists on the 2nd week of the postoperative period.
Levels of TNF-α, IL-6 and IL-8 are known to serve as markers of systemic chronic inflammation. Each of them showed a relationship with long-term survival after surgery. Survival in cancer patients with multiorgan resections demonstrated dependence on the serum levels of circulating TNF-α, IL-6 and IL-8. In the group of L-ornithine L-aspartate therapy with a combination of quercetin and povidone, the indicators of systemic chronic inflammation were lowest and overall survival was better.
Conclusions
In patients with multiorgan resections, significant violations of protein metabolism were detected with an increase in prooxidant processes, manifested itself by an increase in the products of oxidative modification of proteins in the preoperative period, followed by a decrease on the 4th day and the 2nd week of the postoperative period, in both spontaneous and induced reactions. During perioperative intensive care, we observed a significant decrease in all the links of the oxidative modification of proteins postoperatively, indicating increased antioxidant protection.
In patients with multiorgan resections, significant violations of the enzymatic state and lipid peroxidation with increased prooxidant processes were revealed, which manifested as an increase in prooxidant enzymes and nitrite-dependent metabolites in the preoperative period with a subsequent increase on the 4th day and the 2nd week of the postoperative period. These changes were significantly minor and fleeting. When conducting our perioperative intensive care, we noted a significant increase in the activity of antioxidant enzymes and a decrease in metabolites of lipid peroxidation, which indicates an increase in antioxidant protection against the background of the use of these agents and the activation of the body’s adaptation reserves. This gives us the basis for the introduction of this therapy in all patients during multiorgan resections.
Overall survival in cancer patients with multiorgan resections revealed a dependence on the levels of circulating TNF-α, IL-6 and IL-8. In the group of L-ornithine L-aspartate and quercetin combination with povidone, the lowest indicators of markers of systemic chronic inflammation and better overall survival were found.
Received 02.04.2021
Revised 16.04.2021
Accepted 20.04.2021

/86.jpg)
/87.jpg)
/87_2.jpg)
/88.jpg)