
Международный неврологический журнал Том 16, №1, 2020
Вернуться к номеру
Концентрація алюмінію та свинцю в сироватці крові потерпілих на мирній території з черепно-мозковою травмою легкого й середнього ступеня тяжкості в гострому і проміжному періодах
Авторы: M.G. Semchyshyn, V.M. Shevaga
Danylo Halytsky Lviv National Medical University, Lviv, Ukraine
Рубрики: Неврология
Разделы: Клинические исследования
Версия для печати
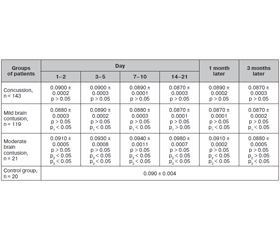
Актуальність. Патогенез черепно-мозкової травми (ЧМТ) багатогранний і значною мірою зумовлений розвитком ендогенної інтоксикації, що веде до накопичення в організмі різних проміжних і кінцевих продуктів метаболізму, у тому числі й токсичних металів. Розуміння основних шляхів патогенезу інтоксикації алюмінієм і свинцем дозволить розробити методи ранньої діагностики, а також дієві заходи з профілактики та лікування. Мета роботи: вивчити зміни показників алюмінію й свинцю в сироватці крові потерпілих мирної території з ЧМТ легкого й середнього ступеня тяжкості в гострому й проміжному періодах. Матеріали та методи. Проведене визначення вмісту алюмінію й свинцю в сироватці крові в 283 потерпілих мирної території з ЧМТ методом атомно-абсорбційної спектрофотометрії з використанням повітряно-ацетиленового полум’я. Результати. З огляду на наявні зміни вмісту токсичних мікроелементів у сироватці крові потерпілих мирної території з ЧМТ легкого й середнього ступеня тяжкості в гострому й проміжному періодах можна стверджувати про наявність у них метаболічних порушень у тканині мозку, пригнічення ендотеліальної функції судин і посилення процесів апоптозу. На нашу думку, у вказаних пацієнтів ендотеліальна дисфункція може розглядатися як маркер судинної патології. Висновки. Таким чином, дослідження вмісту токсичних мікроелементів у сироватці крові потерпілих мирної території з ЧМТ легкого й середнього ступеня тяжкості в гострому й проміжному періодах можуть бути використані як діагностичний і прогностичний критерії перебігу травматичної хвороби головного мозку та в експертних цілях, а вивчення основних шляхів патогенезу алюмінієвої та свинцевої інтоксикації дозволить розробити методи їх ранньої діагностики, дієві заходи з профілактики й лікування.
Актуальность. Патогенез черепно-мозговой травмы (ЧМТ) многогранный и в значительной степени обусловлен развитием эндогенной интоксикации, которая приводит к накоплению в организме различных промежуточных и конечных продуктов метаболизма, в том числе и токсических металлов. Понимание основных путей патогенеза интоксикации алюминием и свинцом позволит разработать методы ранней диагностики, а также действенные меры по профилактике и лечению. Цель работы: изучить изменения показателей алюминия и свинца в сыворотке крови потерпевших на мирной территории с ЧМТ легкой и средней степени тяжести в остром и промежуточном периодах. Материалы и методы. Проведено определение содержания алюминия и свинца в сыворотке крови у 283 потерпевших на мирной территории с ЧМТ методом атомно-абсорбционной спектрофотометрии с использованием воздушно-ацетиленового пламени. Результаты. С учетом очевидных изменений содержания токсических микроэлементов в сыворотке крови потерпевших на мирной территории с ЧМТ легкой и средней степени тяжести в остром и промежуточном периодах можно говорить о наличии у них метаболических нарушений в ткани мозга, угнетении эндотелиальной функции сосудов и усилении процессов апоптоза. По нашему мнению, у указанных пациентов эндотелиальная дисфункция может рассматриваться как маркер сосудистой патологии. Выводы. Таким образом, исследования содержания токсических микроэлементов в сыворотке крови потерпевших на мирной территории с ЧМТ легкой и средней степени тяжести в остром и промежуточном периодах могут быть использованы в качестве диагностического и прогностического критериев течения травматической болезни головного мозга и с экспертными целями, а изучение основных путей патогенеза алюминиевой и свинцовой интоксикации позволит разработать методы их ранней диагностики, действенные меры по профилактике и лечению.
Background. Pathogenesis of the traumatic brain injury is multifaceted and is largely dependent on the development of endogenous intoxication, which leads to the accumulation of various intermediate and end products of metabolism, including toxic metals, in the body. Understanding the basic pathways of the pathogenesis of aluminium and lead intoxication will allow developing the early diagnostic methods as well as effective preventive and treatment measures. The paper aimed to study changes in blood serum concentration of aluminium and lead in persons from the peaceful territory with mild to moderate traumatic brain injury in acute and intermediate periods. Materials and methods. The blood serum concentration of aluminium and lead in 283 people of the peaceful territory with traumatic brain injury of mild to moderate severity in acute and intermediate periods was determined by atomic absorption spectrophotometry using an air-acetylene flame. Results. Given the changes in the content of toxic trace elements in the blood serum of people of the peaceful territory with traumatic brain injury of mild to moderate severity in the acute and intermediate periods, it can be argued that they have metabolic disorders in the brain tissue, inhibited endothelial function of the vessels and intensification of the apoptosis processes. In our opinion, endothelial dysfunction in these people of the peaceful territory may be considered as a marker of vascular pathology. Conclusions. Thus, the study of toxic trace elements in the blood serum of people of the peaceful territory with traumatic brain injury of mild to moderate severity in the acute and intermediate periods can be used as diagnostic and prognostic criteria for the course of traumatic brain disease and for expert purposes, and the study of the major pathways of pathogenesis of aluminium and lead intoxication will allow developing the methods for their early diagnosis, effective measures of prevention and treatment.
алюміній; свинець; черепно-мозкова травма
алюминий; свинец; черепно-мозговая травма
aluminium; lead; brain injury
Introduction
Materials and methods
Results and discussion
/25.jpg)
/26.jpg)
Conclusions
Prospects for further investigation
1. Бойченко П.К., Лузин В.И., Хорькова Е.А. и др. Влияние алюминия на обмен биоминералов. Укр. морфологический альманах. 2006. 4(2). 120-121.
2. Волошин П.В., Малахов В.А., Завгородняя А.Н. Эндотелиальная дисфункция при церебральной патологии. Харьков: Украина, 2006. 92 с.
3. Кудрин А.В., Громова О.А. Микроэлементы в неврологии М.: ГЭОТАР-Медиа, 2006. 304 с.
4. Зербино Д.Д., Соломенчук Т.М., Поспишиль Ю.А. Свинец — этиологический фактор поражения сосудов: основные доказательства. Архив патологии. 1997. 59(1). 9-12.
5. Текуцкая Е.Е., Софьина Л.И., Бендер Л.В., Онищенко Н.П. Методы и практика контроля содержания тяжелых металлов в биосредах. Гигиена и санитария. 1999. 4. 72-74.
6. Штабский Б.М., Гжегоцкий М.Р. Профилактическая токсикология и прикладная физиология: общность проблем и пути решения. Львов: НАУТИЛУС, 2003. 342 с.
7. Тайцлин В.И. Закрытая черепно-мозговая травма и ее последствия. Междунар. мед. журнал. 2002. 1–2. 58-62.
8. Педаченко Є.Г., Шлапак І.П., Гук А.П., Пилипенко М.М. Черепно-мозкова травма: сучасні принципи невідкладної допомоги: навч.-метод. посібник. К.: ВАРТА, 2007. 312 с.
9. Апихтіна О.Л., Коцюруба А.В., Коркач Ю.П. та ін. Вазотоксична дія свинцю: роль порушень в системі оксиду азоту. Укр. журн. з проблем медицини праці. 2007. 3(11). 56-62.
10. Зенков Н.К., Ланкин В.З., Меншикова Е.Б. Окислительный стресс. Биохимический и патофизиологический аспекты. М.: МАИК «Наука-Интерпериодика», 2001. 343 с.
11. Живолупов С.А., Самарцев И.Н., Коломенцев С.В. Опыт применения препарата «Аксамон» в комплексной терапии больных с черепно-мозговыми травмами в восстановительном периоде. Российский национальный конгресс «Человек и лекарство». М., 2009. 100-101.
12. Davidson T., Ke Q., Costa M. Transport of Toxic Metals by Molecular/Ionic Mimicry of Essential Compounds. In Handbook on the toxicology of metals. 3rd ed. Ed. by Nordberg G.F. et al. Acad. Press, London New York Tokyo, 2007. P. 79-84.
13. Prozialeck W.C., Edwards J.R., Nebert D.W. et al. The Vascular System as a Target of Metal Toxicity. Toxicological Sciences. 2008. 102(2). 207-18.
14. Rapoport M.J., McCullagh S., Shammi P. et al. Cognitive impairment associated with major depression following mild and moderate traumatic brain injury. The Journal of Neuropsychiatry and Clinical Neurosciences. 2005. 17. 61-5.