Introduction
The Hashimoto’s encephalopathy (HE) is a rare autoimmune neuroendocrine syndrome associated with a high titer of the antithyroid antibodies [1, 2, 4]. Distinctive feature of HE is a positive response to the treatment with corticosteroids; thus, the syndrome has the second name — a steroid-responsive encephalopathy associated with an autoimmune thyroiditis (SREAT). In 1966, English neurologist Brain [6] has first described a patient suffering from an autoimmune thyroiditis with transient episodes of a hemiplegia, convulsive attacks with confused consciousness and vision disorders. Since the interrelation between a high concentration of the antithyroid antibodies and neurologic symptoms has been determined for the first time, the research of these antibodies level in all cases of idiopathic encephalopathies was offered. Some authors suggest that HE may manifest in autoimmune cerebral vasculitis [16]. According to literature data, the prevalence of HE is 2.1 per 100,000 population. Average age of the disease onset is 44 years, women suffer 4–5 times more often than men. We reviewed the literature sources and revealed the prevalence of clinical implications of the HE to be as follows: rest tremor (84 %), seizure (66 %), epileptic status (12–20 %), transient aphasia (73 %), hypersomnia (63 %), dynamic ataxia (63 %), myoclonias (38 %), depression of cognitive functions (36 %), alienations (36 %) [1, 3, 14].
Because of lack of accurate diagnostic criteria, variety of the clinical manifestations imitating a picture of various neurologic and psychiatric disorders, HE often remains undiagnosed [8]. One of the leading mechanisms in formation of EH and its manifestations is disturbance of the hematoencephalic barrier, due to the development of the T-cellular lymphocytic vasculopathy against the background of an autoimmune reaction of antithyroid antibodies against brain cells [9, 10]. We did not find the detailed clinical description of seizure features in HE picture presented in literature sources. We carried out a clinical trial of neurologic disturbances in HE; the EEG and MRI researches were performed while diagnosing. On the basis of the results, the correlation of neurologic disorders with encephalopathy intensity and severity of a patient’s condition was determined.
Purpose: to specify clinical, neuroimaging, immunologic, neurophysiological features of Hashimoto’s encephalopathy on the basis of a clinical case to increase the efficiency of diagnosis of this infrequent disease.
Case presentation
The patient is a Caucasian woman of 44 years old, admitted to the regional hospital neurology unit on the 10th day from the disease onset with complaints about headache and general weakness. From the medical history it was known that 10 days prior to the consultation the patient experienced severe alalia as paraphasia. The patient was taken to the hospital, where she had the first convulsive attack with consciousness disturbance, which manifested with tonic and clonic cramps. Standard MRI of the brain, lumbar puncture were performed. After the complaints and disease history collecting, differential diagnoses were as follows: disturbance of the cerebral circulation (stroke) or the nervous system infectious lesion (encephalopathy) as the most probable diseases for this patient.
The results of neurological assessments demonstrated negative meningeal signs, the elements of the motor aphasia (paraphasia), the anomy. The patient had a score of 24 on Mini-Mental State Examination. The disturbance of verbal short-term memory was noted. The pupils were equal in size; photoreaction was alive. The nystagmus was horizontal. The strength and the movements of extremities were not affected. The tendon reflexes were high mostly on the left side. There was clonus of the left foot. There were no signs of foot pathology. The sensivity examination was normal. The Romberg test was unstable. The cerebellar test was normal.
The previous diagnoses were assumed: the encephalopathy of unknown origin; the encephalopathy; the system diseases with neurological manifestations.
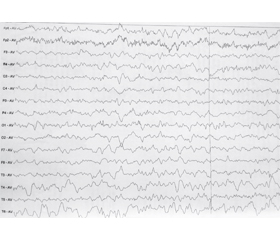
The anticonvulsant therapy (levetiracetam 1000 mg per day), the anti-infectious therapy (valaciclovir 1500 mg per day, cridanimodum 250 mg per day), the metabolic therapy (citicoline 500 mg/day) were prescribed. On the 10th day from the onset of the illness the standard EEG research was conducted. The dominated theta and delta activity slow wave in all leadings, the high-frequency beta activity, single sharp waves with accent in R-leading, the tendency to generalized paroxysms in the theta range were revealed. There was a little alpha rhythm (amplitude was up to 30 mV). The test with hyperventilation was not fully carried out due to deterioration of the patient’s health (Fig. 1).
There were diagnosed the marked changes in the stem structures of the brain (the research was conducted while the anticonvulsant therapy). The medical history reports neither chronic diseases nor surgeries in the past.
On the 15th day of the disease, the patient’s health condition didn’t improve. Octagam (class G immunoglobulins) and methylprednisolone at a dose of 1000 mg per day were added to the treatment scheme. Since, the autoimmune encephalopathy was the dominating diagnosis in diagnostic search.
On the 17th day from the disease beginning, the general clinical examination and the US diagnosis of the thyroid gland were performed. In the gland tissues the groups of hypoechoic foci (up to 3.3 mm) and hyperechoic foci (up to 3.3 mm) in the right lobe were found. The appearance of isoechoic foci about 10 × 8 mm was revealed with a hypoechoic contour in the left lobe. The blood was taken to determine the thyroid gland hormones because of the presence of structural changes in thyroid parenchyma on the 18th day from the illness onset. Also, MRI of the brain with contrast agent was carried out. The foci of a high MR-signal about 1 × 2 mm, mainly in basal ganglia, were found on series of MR-tomograms in the sagittal, axial and coronary projection in T1, T2, T2-FLAIR MR-images. Pathological accumulation of paramagnetic contrast agent was not found after the contrast had been introduced (Fig. 2, 3).
/76.jpg)
At the same day, the patient was examined by an endocrinologist, and the diagnosis “The chronical autoimmune thyroiditis, the diffuse and nodular, with hypothyrosis” was determined. Nodular goiter on the right part. The Table 1 demonstrates the blood tests results for thyroid gland hormones on the 18th day from the illness onset.
The steroid therapy caused the neurologic symptoms regression. So, the clinical picture, disease development, neuroimaging data and electrophysiologic methods, la-boratory analyses data and corticosteroid therapy response made HE possible to be diagnosed.
During survey, when the patient was discharged from the hospital, the patient experienced normal consciousness and was contactable. The speech demonstrated no elements of either aphasia or dysarthria. The patient had a score of 28 on the Mini-Mental State Examination.
The verbal short-term memory was normal. Meningeal signs were negative. The pupils were equal; photoreaction was alive. There was end-point horizontal nystagmus. The strength and the movements in extremities were unaffected. The tendon reflexes were slightly raised on the left side. There were no signs of foot pathology. The sensitivity examination was normal. The Romberg test was stable. The coordination tests were good.
We reported the clinical case of the 44-year-old Caucasian woman with HE (verified as a result of diagnostic process) in the form of tonic-clonic cramps. The patient was not informed that she suffered from a thyroiditis.
/76_2.jpg)
In the early terms from the beginning of clinical manifestations (the 3rd day), the emergence of symptoms of partial motor and sensory aphasia with expressive language disorders, elements of semantic aphasia, verbal paraphasia, acalculia, impaired verbal short-term memory were noted. The patient experienced a score of 24 on MMSE at the disease onset, and 28 after the correct diagnosis was determined and following treatment was performed. The tendon reflexes (the biceps reflex, brachioradialis reflex, knee reflex) expressively raised on the left side, there is clonus of the left foot without decrease in muscular power of the left limbs. The treatment of herpes viral encephalitis as the most probable disease within 10 days was carried out because the patient had IgG to herpes simplex virus type 1, 2. After verification of HE diagnosis and prescription of corticosteroids (methylprednisolone at a dose of 1000 mg per day) the condition of the patient considerably improved with pyramidal, speech, cognitive symptoms and seizures regression. This case shows the need of differential diagnosis while taking into account the probability of HE with a combination of the seizures, thyroidopathy, non-specific focal neurologic symptoms.
But it is necessary to consider that HE, also known as a steroid-responsive encephalopathy associated with an autoimmune thyroiditis (SREAT), can be the weakened reaction of SREAT manifestation, which often is not diagnosed due to the lack of accurate diagnostic criteria. HE is characterized by features of autoimmune disease, found more often among women in comparison with the men [1, 5, 9]. It is represented by variable neurological symptoms, augmentation of antithyroid peroxidase and has a positive response to the corticosteroid therapy [1, 15].
The 44-year-old Caucasian female patient with the verified Hashimoto’s encephalopathy was examined and treated in terms up to 30 days. The MRI of the brain with a contrast agent in T1, T2, FLAIR was performed. Also, there were used the neurophysiological methods of the computer electroencephalography (technique Medic-XAI), the ultrasonography of the thyroid gland, as well as the hormone levels (thyroid-stimulating hormone) and the immunological status (antibody against TPO, T3, T4) were determined.
The assessment of combinations of a clinical picture and probable correlations of these clinical research with the neurological status and the disease course was carried out.
Conclusion
Newly developed seizures without the obvious reason combined with a thyroidopathy, which is followed by impaired hormonal and immunologic status and development of the mild neurological, neuropsychological symptoms, mainly among the women of middle age, can be a manifestation of HE.
Taking into account the need of the exception of close conditions for diagnosing HE, the assessment of antiserum capacities of NMDA, GABA to receptors whose increase accompanies the autoimmune encephalitis more frequent at paraneoplastic processes is desirable.
Existence of chronic autoimmune thyroiditis verified by the structural changes of the thyroid gland and increase of antithyroid peroxidase (1126.98 IU/mL; norm up to 100 IU/mL) with significant increase of the thyroid-stimulating hormone level (9.1 μU/mL; norm 0.17–4.05 μU/mL) and clinical assessment of values of free thyroxine and free triiodothyronine were accepted as confirmation of high probability of HE, taking into account the nature of changes of the central nervous system.
The focal changes of the brain and their localization were mild and considered as labile in the described case of HE. They settled mainly in the basal ganglia. The standard computer EEG showed diffuse disorganization of rhythm (with deformation mainly in the pointed peak, multiple sharp-wave complexes, the periods of theta activity patterns of EEG of epileptic character).
Conflicts of interests. Authors declare no conflicts of interests that might be construed to influence the results or interpretation of their manuscript.
Список литературы
1. Riangwiwat T. Steroid-responsive encephalopathy: an under recognised aspect of Hashimoto’s thyroiditis / T. Riangwiwat, J. Sangtian, C. Sriphrapradang // BMJ Case Rep. — 2015. — Mar 12.
2. Gauthier A.C. Hashimoto’s encephalopathy mimicking Creutzfeldt-Jakob disease / A.C. Gauthier, J.M. Baehring // J. Clin. Neurosci. — 2017. — Jan 35. — P. 72-73.
3. González R.P. Autoimmune encephalitis induced by antibodies against GABA receptor / R.P. González, A.L. Hudson, M.E. Basáez, C.M. Miranda // Rev. Med. Chil. — 2016 Nov. — 144 (11). — P. 1491-1493.
4. Kishitani T. Limbic encephalitis associated with anti-NH2-terminal of α-enolase antibodies: A clinical subtype of Hashimoto encephalopathy // T. Kishitani, A. Matsunaga, M. Ikawa, K. Hayashi, O. Yamamura, T. Hamano, O. Watanabe, K. Tanaka, Y. Nakamoto, M. Yoneda // Medicine (Baltimore). — 2017 Mar. — 96(10).
5. Zhu M. Hashimoto’s encephalitis associated with AMPAR2 antibodies: a case report / M. Zhu, X. Yu, C. Liu, C. Duan, C. Li,
J. Zhu, Y. Zhang // BMC Neurol. — 2017 Feb 21. — 17(1). — 37. doi: 10.1186/s12883-017-0823-4.
6. Britton J. Autoimmune epilepsy / J. Britton // Hand Clin. Neurol. — 2016. — 133. — P. 219-45. doi: 10.1016/B978-0-444-63432-0.00013-X. Review.
7. Guan H.Z. Autoimmune Encephalitis: An Expanding Frontier of Neuroimmunology / H.Z. Guan, H.T. Ren, L.Y. Cui // Chin. Med. J. (Engl). — 2016 May 5. — 129 (9). — P. 1122-7.
8. Graham B.R. Hashimoto Encephalopathy Presenting With Stroke-Like Episodes in an Adolescent Female: A Case Report and Literature Review / B.R. Graham, N. Shiff, M. Nour, S. Hasal, R. Huntsman, S. Almubarak // Pediatr. Neurol. — 2016 Jun. — 59. — P. 62-70.
9. Yoneda M. Hashimoto’s encephalopathy / M. Yoneda // Nihon. Rinsho. — 2015 Sep. — 73 Suppl 7. — P. 603-6.
10. Bhoi S.K. Clinical spectrum of Hashimoto encephalopathy: report of 5 cases / S.K. Bhoi, J. Kalita, U.K. Misra // Acta Neurol. Belg. — 2016 Mar. — 116(1). — P. 101-4.
11. Bergink V. Autoimmune Encephalitis in Postpartum Psychosis / V. Bergink, T. Armangue, M.J. Titulaer, S. Markx, J. Dalmau, S.A. Kushner // Am. J. Psychiatry. — 2015 Sep 1. — 172(9). — P. 901-8.
12. Guirgis H. A Case of Hashimoto’s Encephalopathy Presenting With Acute Psychosis / H. Guirgis, C. Amar // J. Neuropsychiatry Clin. Neurosci. — 2014 Fall. — 26(4). — E1-2.
13. Veltman E.M. Hashimoto encephalitis and depression / E.M. Veltman, D. Rhebergen, E. van Exel, M.L. Stek // Tijdschr. Psychiatr. — 2015. — 57 (4). — P. 280-3.
14. Sapkota S.K. Hashimoto encephalopathy or neurosarcoidosis? A case report / S.K. Sapkota, B.L. Sapkota, N. Pitiyanuvath // Neurohospitalist. — 2015 Apr. — 5 (2). — P. 70-3
15. Haider A.S. Autoimmune Schizophrenia? Psychiatric Manifestations of Hashimoto’s Encephalitis / A.S. Haider, M. Alam, E. Adetutu et al. // Cureus. — 2016 Jul 5. — 8 (7). — 672.
16. Farrell R.M. Hashimoto’s encephalopathy: a rare pediatric brain disease / R.M. Farrell, M.B. Foster, A.O. Omoruyi, S.E. Kingery, K.A. Wintergerst // J. Pediatr. Endocrinol. Metab. — 2015 May. — 28 (5–6). — P. 721-4.

/75.jpg)