
Журнал «Боль. Суставы. Позвоночник» Том 8, №3, 2018
Вернуться к номеру
Зв’язок метаболічного синдрому і мінеральної щільності кісткової тканини, показника якості трабекулярної кісткової тканини в жінок у постменопаузальному періоді з невертебральними переломами
Авторы: Vladyslav Povoroznyuk (1), Larysa Martynyuk (2), Iryna Syzonenko (3), Liliya Martynyuk (2)
(1) — State Institution “D.F. Chebotarev Institute of Gerontology of the NAMS of Ukraine”, Kyiv, Ukraine
(2) — State Institution of Higher Education “I. Horbachevsky Ternopil State Medical University”, Ternopil, Ukraine
(3) — Kyiv Municipal Center for Radiation Protection of Citizens Affected by the Chernobyl Disaster, Kyiv, Ukraine
Рубрики: Ревматология, Травматология и ортопедия
Разделы: Клинические исследования
Версия для печати
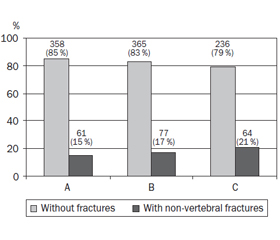
Актуальність. Медична, соціальна й економічна значимість остеопорозу обумовлена зниженням якості життя, збільшенням інвалідності та смертності пацієнтів у результаті переломів, викликаних низькоенергетичною травмою. Мета дослідження: вивчити кореляцію компонентів метаболічного синдрому, мінеральної щільності кісткової тканини (МЩКТ) і показника якості трабекулярної кісткової тканини (trabecular bone score — TBS) у жінок у постменопаузальному періоді з невертебральними переломами. Матеріали та методи. Пацієнтки в постменопаузальному періоді віком 50–79 років (n = 1161) були обстежені і розподілені на три групи: до групи А увійшли 419 жінок із підвищеною масою тіла (індекс маси тіла (ІМТ) — 25,0–29,9 кг/м2), групи Б — 442 жінки з ожирінням (ІМТ > 29,9 кг/м2) і до групи В — 300 жінок із метаболічним синдромом (діагноз установлений відповідно до критеріїв Міжнародної федерації діабету, 2005). Двохенергетична рентгенівська абсорбціометрія (Prodigy, GE Medical systems, Lunar, Madison, WI, USA, 2005) використовувалася для визначення МЩКТ поперекового відділу хребта (L1–L4), шийки стегна, всього скелету і передпліччя і показників якості кісткової тканини (останніх — за допомогою програмного забезпечення Medimaps). Дані аналізувалися за допомогою програми Statistica 6.0. Результати. Значне збільшення МЩКТ поперекового відділу хребта (L1–L4), шийки стегнової кістки, всього скелету і ультрадістального відділу променевої кістки було виявлено в жінок з ожирінням і метаболічним синдромом на відміну від пацієнток із предожирінням (p < 0,001). TBS був значно вищим у жінок із підвищеною масою тіла порівняно з пацієнтками з ожирінням і метаболічним синдромом. Аналіз показав значну позитивну кореляцію між окружністю талії, рівнем тригліцеридів і МЩКТ поперекового відділу хребта і стегнової кістки. Установлений значний негативний зв’язок між рівнем ліпопротеїнів високої щільності (ЛПВЩ) у сироватці крові та МЩКТ досліджуваних ділянок. Висновки. TBS (L1–L4) позитивно корелює з рівнем ЛПВЩ. Незважаючи на те що показники МЩКТ були кращими в жінок із метаболічним синдромом, частота невертебральних переломів у цій групі була значно вищою.
Актуальность. Медицинская, социальная и экономическая значимость остеопороза обусловлена снижением качества жизни, увеличением инвалидности и смертности пациентов в результате переломов, вызванных низкоэнергетической травмой. Цель исследования: изучить корреляцию компонентов метаболического синдрома, минеральной плотности костной ткани (МПКТ) и показателя качества трабекулярной костной ткани (trabecular bone score — TBS) у женщин в постменопаузальном периоде с невертебральными переломами. Материалы и методы. Пациентки в постменопаузальном периоде в возрасте 50–79 лет (n = 1161) были обследованы и разделены на три группы: в группу А вошли 419 женщин с повышенной массой тела (индекс массы тела (ИМТ) — 25,0–29,9 кг/м2), группу Б — 442 женщины с ожирением (ИМТ > 29,9 кг/м2) и в группу В — 300 женщин с метаболическим синдромом (диагноз установлен согласно критериям Международной федерации диабета, 2005). Двухэнергетическая рентгеновская абсорбциометрия (Prodigy, GE Medical systems, Lunar, Madison, WI, USA, 2005) использовалась для определения МПКТ поясничного отдела позвоночника (L1–L4), шейки бедренной кости, всего скелета и предплечья и показателей качества костной ткани (последних — с помощью программного обеспечения Medimaps). Данные анализировались с помощью программы Statistica 6.0. Результаты. Значительное увеличение МПКТ поясничного отдела позвоночника (L1–L4), шейки бедренной кости, всего скелета и ультрадистального отдела лучевой кости было обнаружено у женщин с ожирением и метаболическим синдромом в отличие от пациенток с предожирением (p < 0,001). TBS был значительно выше у женщин с избыточной массой тела по сравнению с пациентками с ожирением и метаболическим синдромом. Анализ показал значительную положительную корреляцию между окружностью талии, уровнем триглицеридов и МПКТ поясничного отдела позвоночника и бедренной кости. Установлена значительная отрицательная связь между уровнем липопротеинов высокой плотности (ЛПВП) в сыворотке крови и МПКТ исследуемых участков. Выводы. TBS (L1–L4) положительно коррелирует с уровнем ЛПВП. Несмотря на то что показатели МПКТ были лучше у женщин с метаболическим синдромом, частота невертебральных переломов в этой группе была значительно выше.
Background. Medical, social and economic relevance of osteoporosis is caused by reducing quality of life, increasing disability and mortality of the patients as a result of fractures due to the low-energy trauma. This study is aimed to examine the associations of metabolic syndrome components, bone mineral density (BMD) and trabecular bone score (TBS) in menopausal women with non-vertebral fractures. Materials and methods. 1161 menopausal women aged 50–79 years were examined and divided into three groups: group A included 419 women with increased body weight (body mass index (BMI) — 25.0–29.9 kg/m2), group B — 442 females with obesity (BMI > 29.9 kg/m2) and group C — 300 women with metabolic syndrome (diagnosis according to International Diabetes Federation criteria, 2005). Dual-energy X-ray absorptiometry (Prodigy, GE Medical systems, Lunar, Madison, WI, USA, 2005) was used for measuring lumbar spine (L1-L4), femoral neck, total body and forearm BMD and bone quality indexes (last using Medimaps software). Data were analyzed using Statistica 6.0 package. Results. A significant increase of lumbar spine (L1-L4), femoral neck, total body and ultradistal radius BMD was found in women with obesity and metabolic syndrome compared to the pre-obese ones (p < 0.001). TBS was significantly higher in women with increased body weight compared to obese and metabolic syndrome patients. Analysis showed a significant positive correlation between waist circumference, triglycerides level and BMD of lumbar spine and femur. Significant negative association was found between serum high-density lipoproteins (HDL) level and BMD of investigated sites. Conclusions. The TBS (L1-L4) indexes positively correlated with HDL level. Despite the fact that BMD indexes were better in women with metabolic syndrome, the frequency of non-vertebral fractures was significantly higher in this group of patients.
мінеральна щільність кісткової тканини; показник якості трабекулярної кісткової тканини; метаболічний синдром; перелом
минеральная плотность костной ткани; показатель качества трабекулярной костной ткани; метаболический синдром; перелом
bone mineral density; trabecular bone score; metabolic syndrome; fracture
Introduction
Materials and methods
Results and discussion
/9-1.jpg)
/10-1.jpg)
/11-1.jpg)
/12-1.jpg)
/12-2.jpg)
Conclusions
- Bliuc D, Nguyen ND, Milch VE, Nguyen TV, Eisman JA, Center JR. Mortality risk associated with low-trauma osteoporotic fracture and subsequent fracture in men and women. JAMA. 2009 Feb 4;301(5):513-21. doi: 10.1001/jama.2009.50.
- Dennison EM, Syddall HE, Aihie Sayer A, Martin HJ, Cooper C; Hertfordshire Cohort Study Group. Lipid profile, obesity and bone mineral density: the Hertfordshire Cohort Study. QJM. 2007 May;100(5):297-303. doi: 10.1093/qjmed/hcm023.
- Hans D, Goertzen AL, Krieg MA, Leslie WD. Bone Microarchitecture Assessed by TBS Predicts Osteoporotic Fractures Independent of Bone Density: The Manitoba Study. J Bone Miner Res. 2011 Nov;26(11):2762-9. doi: 10.1002/jbmr.499.
- Gonelli S, Caffarelli C, Nuti R. Obesity and fracture risk. Clin Cases Miner Bone Metab. 2014 Jan;11(1):9-14. doi: 10.11138/ccmbm/2014.11.1.009.
- Huang CY, Liao LC, Tong KM, et al. Mediating effects on health-related quality of life in adults with osteoporosis: a structural equation modeling. Osteoporos Int. 2015 Mar;26(3):875-83. doi: 10.1007/s00198-014-2963-3.
- International Diabetes Federation. IDF Consensus Worldwide definition of the metabolic syndrome. Available from: https://www.idf.org/e-library/consensus-statements/60-idfconsensus-worldwide-definitionof-the-metabolic-syndrome.html. Accessed: August 24, 2005.
- Sun K, Liu J, Lu N, Sun H, Ning G. Association between metabolic syndrome and bone fractures: a meta-analysis of observational studies. BMC Endocr Disord. 2014 Feb 9;14:13. doi: 10.1186/1472-6823-14-13.
- Maghraoui A, Rezqi A, Mrahi S, Sadni S, Ghozlani I, Mounach A. Osteoporosis, vertebral fractures and metabolic syndrome in postmenopausal women. BMC Endocr Disord. 2014 Dec 10;14:93. doi: 10.1186/1472-6823-14-93.
- von Muhlen D, Safii S, Jassal SK, Svartberg J, Barrett-Connor E. Associations between the metabolic syndrome and bone health in older men and women: the Rancho Bernardo Study. Osteoporos Int. 2007 Oct;18(10):1337-44. doi: 10.1007/s00198-007-0385-1.
- International Society for Clinical Densitometry. 2007 ISCD Official Positions. Available from: https://www.iscd.org/official-positions/official-positions/. Accessed: October 2007.
- Poiana C, Carsote M, Radoi V, Mihai A, Capatina C. Prevalent osteoporotic fractures in 622 obese and non-obese menopausal women. J Med Life. 2015 Oct-Dec;8(4):462-6.
- Ott SM. Bone strength: more than just bone density. Kidney Int. 2016 Jan;89(1):16-9. doi: 10.1016/j.kint.2015.11.004.
- Muka T, Trajanoska K, Kiefte-de Jong JC, et al. The Association between Metabolic Syndrome, Bone Mineral Density, Hip Bone Geometry and Fracture Risk: The Rotterdam Study. PLoS One. 2015 Jun 12;10(6):e0129116. doi: 10.1371/journal.pone.0129116.
- World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation on obesity. Geneva: World Health Organization; 2000. 252 p. Available from: http://www.who.int/nutrition/publications/obesity/WHO_TRS_894/en/.
- Yang L, Lv X, Wei D, Yue F, Guo J, Zhang T. Metabolic syndrome and the risk of bone fractures: A Meta-analysis of prospective cohort studies. Bone. 2016 Mar;84:52-56. doi: 10.1016/j.bone.2015.12.008.