Статтю опубліковано на с. 13-19
Investigating quality of life (QOL) is increasingly being used in clinical medicine as it lets, on the one hand, study the disease influence on different constituents of patient’s health, and, on the other hand, detect additional advantages or disadvantages of an ongoing therapy. Introducing modern technologies of researching quality of life into clinical practice opened an access to the important information on patient’s functioning spheres that is used both for developing treatment and rehabilitation programmes and for monitoring the level of patient’s health during treatment [17].
The problem of improving quality of life in neurologic di–seases, especially in epilepsy, still remains urgent. It is explained by the fact that epilepsy is one of the most important diseases from medical and psychological and social views. There are nearly 50 million epilepsy patients in the world, 5 % of the population suffer at least one seizure in their lifetime, in 20–30 % of patients this disease is lifelong [22]. According to WHO, more than 75 % and, according to the Russian analysis, nearly 63 % of registered patients do not get a rational antiepileptic therapy [5, 12, 14, 15].
Nowadays the strategy of treating epilepsy has undergone significant changes. The modern approach to the problem of treating epilepsy provides the solution of a number of issues for not only to achieve a maximum therapeutic effect but for adequate and comfortable functioning of patients in a society (getting an education, occupational choice, employment, family). In the middle of the last century the treatment prio–rity was to eliminate attacks and psychoemotional disorders, at the present stage, the priority is a patient, and the goal is to improve a quality of life [23]. According to the World Health Organization definition, QOL is people’s perception of their life status in the context of cultural and value orientations in line with their own goals, expectations, standards and concerns [1]. QOL is defined as a person’s contentment with his/her physical, psychic and social wellbeing in all aspects of his/her functioning in a society [2].
Numerous studies have found a significant deterioration in QOL in patients with epilepsy compared to the rest of a population [18]. The factors decreasing QOL are quite diverse. Often the mere diagnosis of epilepsy is dramatic for a patient, causing social disadaptation, contributing to psychological distress and reduced QOL [22]. Epileptic seizures, the fear of their recurrence and the attitude of people around influence negatively as well [26]. The increased risk of psychic and cognitive disorders, damage to physical health is associated just with seizures [23]. The necessity of prolonged antiepileptic drugs (AEDs) taking appears to be one of the most significant negative factors which itself can reduce QOL causing psychic and cognitive disorders and affect a disease course and the severity of seizures.
At the same time pharmacotherapy achievements have not resulted in significant changes in social status of epileptic patients that is due to the ongoing stigmatization of these persons by the society. The society is not ready yet to accept the fact that epilepsy can be cured. In the modern society, these patients are still subjected to social discrimination and active social and labor abridgements contradicting their real abilities. There are legislative regulations significantly limi–ting a social activity even in the most developed countries, resulting in social disadaptation and isolation [16]. Quite often patients have difficulty not so much connecting to their disease as connecting to a poor society orientation in. It is stigma (segregating an individ according to any negative property) that is considered to be a main obstacle for bettering quality of life of psychoneurological patients [7, 9].
Thus, the challenge of epileptic patients’ QOL is connected not only to disease clinical manifestations but to a personal reaction to it, to the necessity to take medicine constantly, to the society attitude which not always reasonably limits their pursuit to a social activity as well. Improving QOL and rehabilitation of epileptic patients is one of the priority goals of modern epileptology [1, 10].
The disease itself and its pharmacotherapy adversely affect different aspects of life. The necessity of prolonged AEDs ta–king, sometimes a low therapy efficacy, changing antiepileptic drugs negatively influences patients’ psychological condition. Despite the fact that the majority of patients being rationally treated have a favorable prognosis, 30 % of patients fail to achieve remission, it impairs life quality and health in whole [20]. Early conducted researches demonstrated that higher life quality indices had been got in the lack of seizures but remission was an insufficient condition of good quality of life. Mood and emotional background significantly influence quality of life as well [19]. Inadequately diagnosing epilepsy and a seizure type, prescribing AED without taking into account a patient’s condition and the presence of comorbid somatic pathology can result in worsening life quality. Anticonvulsants side effects unfavorably bias life quality as well [4, 11].
At present the interest in brain stimulation methods as an alternative therapy of epilepsy is increasing as a number of patients have refractory to antiepileptic drugs. Furthermore, not all the patients with this pathology can undergo a surgical treatment. Currently, vagus nerve stimulation, deep brain electrical stimulation, micropolarization and repeated transcranial magnetic stimulation (rTMS) present brain stimulation methods [6, 26, 25]. The data about the rTMS ability to decrease motor cortex excitability and to become a perspective method of treating patients with epilepsy were a precondition for therapeutic using magnetic stimulation.
Studying the quality of life of epilepsy patients is important in assessing a treatment efficacy as well as in comparing effectiveness of different kinds of therapy of this disease. The information about life quality indices at using therapeutic rTMS is not available in scientific literature. That is why one of our study tasks was the assessment of changing quality of life of epilepsy patients after a combined therapy with low doses of anticonvulsants and rTMS.
Materials and Methods
We examined 48 patients with epilepsy (27.60 ± 0.99 years). The disease length from a debut was 15.1 ± 1.4 years.
Inclusion criteria were a reliable diagnosis defining epileptic syndrome and seizure type in accordance with the recommendations of the International League against Epilepsy as well as the necessity to decrease AEDs doses to subtherapeutic and the absence of absolute contraindications to rTMS (metal clips in brain tissues, an electronic heart pacemaker and other pacemakers).
All patients underwent a course of therapeutic rTMS. Exposure to a pulsed magnetic field was carried out over an area of the projection of brain temporal lobe using a coil IR 02–150 of a magnetic stimulator Neuro-MS. The side for stimulation was defined depending on the results of a clinical examination, MRI and EEG. TMS was performed with a pulsed magnetic field with biphasic pulses of 250 ms duration with an interval of 1 s between pulse packs and the pack duration of 10 s. The stimulation frequency of 1 Hz at the intensity of pulsed magnetic field of 20 % of maximum magnetic induction was used. The session duration was 10 minutes, the course of in-patient treatment was 10 daily procedures.
All the examined patients had polymorphic seizures which were a combination of simple, complex partial and generalized seizures.
The peculiarity of sample group was a relatively young age, the lack of mental disorders, the social adaptation of patients which had a permanent job or successfully study at a high school or a college.
The examination included: history taking, clinical, neurological examination of a patient, analyzing seizures frequency and anticonvulsants side-effects, diffuse tensor MRI of brain with tractography, EEG mapping, registering cognitive evoked potential P 300, assessing quality of life on QOLIE‑31, assessing seizures severity according to SSQ (Seizure Severity Questionnaire), objectifying comorbid anxiety and depressive disorders according to Beck depression scale and Spielberger — Khanin anxiety scale. Analyzing results of QOL assessment was performed according to QOLIE‑31 at the following control points: before the therapy, in a month and in 3 months after a therapy start.
Neuropsychological testing on the questionnaire QOLIE‑31 (Quаlity of Life in Epilepsy Inventory‑31) lets quantitatively assess a general score and 7 main QOL spheres of an epilepsy patient: fear of seizures, general QOL, emotional well-being, activity/fatigability, cognitive functioning, drugs influence, social functioning [18].
For statistic manipulations we used the algorithms of the programme Statistica 6.0. To assess nonparametric results we used the Wilkinson criterion, qualitative parameters — the Fisher criterion. Correlation analysis was performed using Spearman’s rank correlation coefficient. The results are given at the level of significance р < 0.05.
Results
Studying dynamics of changes has shown that QOL of epilepsy patients is a systemic characteristic and depends on a number of clinical, psychoemotional and social factors.
Seizure frequency is an important factor of decreasing QOL (r = –0.41; t = –2.38; p = 0.024), as well as their severity by SSQ (r = –0.55; t = –3.45; p = 0.0018).
Patients with frequent seizures worse evaluated the quality of their lives, it indicates their dominant role in maladjustment in epilepsy.
While analyzing QOL indices depending on a seizure type, lower indices (due to a low assessment of the items «cognitive function» and «drug effects») were significantly obtained in patients with partial seizures prevailing (r = –0.36; t = –2.1; p = 0.044). We can assume that partial seizures lead to a lower satisfaction with the major areas of their lives that is associated with the experience of negative attitudes towards their state. Partial seizures with a change in consciousness are often accompanied by inadequate or even asocial behavior of patients causing confusion or even a negative reaction of others that brings a significant moral damage causing severe mental suffe–ring, enhancing the subjective dissatisfaction with their lives. We revealed a tendency to a lower assessment of QOL on the item «cognitive function» r = 0.38; t = 2.2; p = 0.036) in patients with a combination of simple and complex partial with generalized tonic-clonic seizures that is a reflection of disease course severity.
It should be noted that the patients in the clinical presentation of which pure absences prevailed more highly evaluated the item «social functioning» (r = 0.35; t = 2.05; p = 0.049).
In case of an organic brain damage due to a perinatal pathology we observed a decrease in the total score of QOL due to a low rating of «drug effects» (r = 0.44; t = 2.68; p = 0.011). The obtained result can be explained by a more complicated course of epilepsy especially in the presence of mesial temporal sclerosis.
No correlation of QOL and disease duration, debut age, delayed therapy, comorbid diseases and pernicious habits as well as gender and age differences was revealed in our study (p > 0.05) [3].
We identified a correlation of decreasing the score of the item «activity/fatiguability» at the debut of a disease with gene–ralized convulsive attacks (r = 0.36; t = 2.09; p = 0.045), of the item «drug effects» in case of relapses after discarding an AED in past history (r = 0.36; t = 2.09; p = 0.045) which is probably connected to AED side-effects making patients discard drugs themselves.
Irregular taking anticonvulsive drugs in past history correlated with a low total percentage of QOL value (r = 0.43; t = 2.55; p = 0.016), the same association was also found in case of irrational polytherapy (r = 0.36; t = 2.07; p = 0.047).
To our point of view, the absence of a correlation to characteristics of EEG mapping reflecting the activity and severity of an epileptic process (р > 0.05) is important as it underlines the dominant role of social and psychological factors in forming a QOL value in epilepsy.
The results of analyzing QOL indices depending on the presence or absence of side-effects of AED therapy showed that the presence of side-effects identified lower QOL indices (r = –0.38; t = –2.17; p = 0.038). In the patient group where topiramate in a combination with a prolonged form of valproate was used, the high QOL level (the items «fear of seizures», «emotional well-being», «activity/ fatigability» and «social functioning») can be explained by a good tolerance to an AED combination at low doses and by the effect of simultaneous drugs influence on different mechanisms of epileptogenesis as well as by favorable effect of rTMS (r = 0.47; t = 2.8; p = 0.009). The topiramate monotherapy was characterized by a high value of overall QOL, emotional well-being, cognitive and social functioning as well (r = 0.47; t = 2.8; p = 0.009). For the sodium valproate monotherapy, no significant correlation with QOL was revealed (р > 0.05).
The factors connected not only to a treatment but to a social status of patients as well are known to have a psychotraumatic effect. Meanwhile there was a correlation of a low total QOLIE‑31 score and a higher education (r = 0.37; t = 2.12; p = 0.043), it is evidence of a dominant influence of disease recognition and patients’ attitude to their disease on their life quality (auto-stigmatization). We found a higher fear of seizures in persons studying at high schools (r = 0.38; t = 2.22; p = 0.034), it is quite understandable as the occurrence of an attack could affect future relations with fellow students and a subsequent employment at distributing at the end of training.
We analyzed QOL indices of epilepsy patients depending on a work status which showed that patients placed in a job had a higher total QOLIE‑31score (r = 0.46; t = 2.76; p = 0.009). In this patients subgroup, the score of the items «overall quality of life», «emotional well-being», «activity/fatigability», «cognitive functions», and «social functioning» was significantly higher compared to unemployed (р < 0.05).
In the group, 5 patients had a disability. QOL values in disabled persons did not differ from that of non-disabled ones (p > 0.05). This can be explained by the fact that in our group all disabled had a permanent job. In other studies, the disabled persons lower evaluated QOL compared to non-disabled ones [12].
22 (45.8 %) patients of the study group were married. Significantly higher QOL indices were obtained in unmarried persons (r = –0.41; t = –2.44; p = 0.02). These results can be associated with a negative experience of surrounding people reaction to the disease including members of their families. However, in case of the support from relatives and/or spouses, the patients significantly higher assessed QOL regardless of whether they were officially married or not (r = 0.61; t = 4.15; p = 0.000265). Social support should be noted to have a mean correlation to QOL value. In this regard, our patients were provided with an access to medical consultative help and a communication via mobile apparatuses and Internet sources for their psychological support.
In the group of patients, with whom regular talks explai–ning disease peculiarities and remission possibility under certain conditions were held, the positive mood was kept, the perspectives of getting education, marriage were discussed, and higher QOL scores were obtained.
A strong correlation of QOL decreasing in all items of QOLIE‑31 was detected in patients with depression (r = –0.76; t = –6.29; p = 0.000001), at high personal (r = –0.82; t = –7.8; p = 0.000008) and situational (r = –0.7; t = –5.9; p = 0.000008) anxiety.
Analyzing dynamics of mean QOL indices before and after rehabilitation therapy using rTMS demonstrated a statistically significant increase in overall QOL score (fig. 1).
/13-19/16-1.jpg)
Analyzing QOLIE‑31 questionnaire parameters in a month from the start of a combined therapy showed a significant increase in QOL value on the following values: overall score (р = 0.00003), overall percentage (р = 0.046), fear of seizures (р = 0.000089), overall quality of life (р = 0.000082), activity/fatigability (р = 0.0015), cognitive functioning (р = 0.00013), drug effects (р = 0.0086), social functio–ning (р = 0.0006). The data of parameters of questionnaire QOLIE‑31 in 3 months from the start of a combined therapy using rTMS showed a significant increase in QOL value on all the indices: overall score (р = 0.0005), fear of seizures (р = 0.0056), overall quality of life (р = 0.005), emotional well-being (р = 0.034), activity/fatigability (р = 0.0013), cognitive functioning (р = 0.0013), drug effects (р = 0.0045), social functioning (р = 0.043).
Comparing the QOL results after one, three and six months we detected no significant differences in the items of the questionnaire QOLIE‑31 (р < 0.05), therefore the effect of QOL value bettering after a course of rTMS kept within 3 months of our observation.
QOL bettering after a combined therapy with rTMS is associated with decreasing the number of seizures by 75 % as well as with the antidepressant effect of magnetic stimulation. The values according to Beck scale before a course of rTMS were 6 (1–14) scores. The antidepressant effect of including rTMS was obtained to the tenth procedure of magnetic stimulation and the value on Beck scale was 1.5 (0–9) scores (р = 0.00004). By the end of the first month depressive symptoms were observed only in 3 patients, the total score of depression scale was 2 (0–4) (р = 0.0037).
The significant decrease in anxiety level in 2 months after an rTMS course can explain the fact of bettering the value «emotional well-being» in the QOL assessment (tab. 1).
The results obtained need to be clarified concerning the presence of predictors of maximum efficacy of anticonvulsant action of a repeated transcranial magnetic stimulation. We used logistic regression method in modelling probable outcomes of an rTMS course. The calculation of the odds ratio is a modern data processing technology letting detect subtle relations between phenomena and determine their significant probability.
First of all, it is important to determine clinico-neurophy–siological and neuroimaging predictors the presence of which indicates a high probability of seizures suppression within the first month from the beginning of a combined therapy as a period exceeding more than 3 times the minimum interval between attacks prior to a new therapy as recommended by the International Antiepileptic League [20]. According to the data obtained, 54.2 % of patients (26 of 48) had no attacks within the first month after a combined therapy (p = 0.00001), by the end of the second month — 39.6 % (р = 0.00001), by the end of the third — 33.3 % (р = 0.00001). When observed within 6 months in 10 out of 34 (29.4 %) of the patients, comply with compliance, seizures were not observed (p = 0.0001).
The expected effect within the first month after an rTMS was associated with the number of attacks within a week (not more than 3) prior to a combined therapy (ОR = 12.4, CI 1.6–93.9, р = 0.04).
The important predictor of seizures frequency reduction appeared to be their minimal polymorphism — a combination of not more than 2 types of seizures (OR = 5.58, CI 0.97–31.99, р = 0.04). The combined therapy at the presence of complex partial seizures (ОR = 18.9, CI 4.23–84.47, р = 0.00008) and the disease duration of more than 10 years (OR = 2.68, CI 1.09–6.59, р = 0.02) was the least efficient one [8].
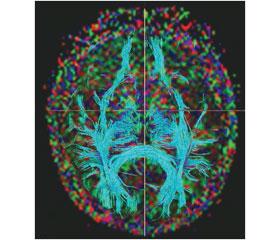
We identified neuroimaging factors providing the proba–bility of seizure frequency reduction, the indices of fractional anisotropy of posterior quadrant of the hemisphere containing an epileptic focus are attributed thereto (OR = 5.58, CI 0.97–31.99, р = 0.03) (fig. 2) [13, 21]. We revealed a tendency to get a combined therapy effectiveness from the normal ratio NAA/(Cho + Cr) in the hippocampus of an opposite hemisphere (OR = 0.02, CI 0.0004–1.33, р = 0.055) (fig. 3).
The indices of neurophysiologic examinations were an important component of effective rTMS, in particular — the integrity of normal values of dominant alpha-rhythm (OR = 0.42, CI 0.18–1.01, р = 0.045) that indicates a relative compensated state of neural activity. Blink reflex characteristics corresponding to its normoexcitable type were associated with a higher pro–bability of appearing the desired result of a combined therapy (OR = 5.66, CI 1.1–29.15, р = 0.032).
Along with sufficient effectiveness of the combined use of AEDs and rTMS, the most pronounced effect was while using drugs blocking voltage-dependent Na+-channels, and the valproates (OR = 1.6, CI 0.79–3.29, р = 0.005) were a leader.
Epileptic activity reduction (OR = 15.7, CI 1.71–144.57, р = 0.012) and tetra-rhythm index decrease (OR = 1.11, CI 1.01–1.23, р = 0.03) on EEG after a single rTMS are predictors of a following successful outcome of a proposed technology.
To reduce seizures frequency by 50 %, a smaller number of predictors are required. The lack of complex partial attacks as before remained an important condition for a success (OR = 18.46, CI 2.00–170.35, р = 0.0083), the polymorphism had no significant association to an outcome, the disease duration more than 15 years hindered in obtaining a desired result (OR = 1.08, CI 1.00–1.16, р = 0.041).
We analyzed the predictors of a combined therapy efficacy in case when seizures reduced within a period of 3 to 6 months after an rTMS. The given result was possible at the lack of complex partial seizures when OR = 2.67 (CI 1.01–7.02, р = 0.04) and disembryogenesis stigmas (short neck, low forehead, widely spaced palpebral fissures, dolichocephaly, etc.) — OR = 2.5 (CI 1.07–5.82, р = 0.029), as well as the lack of carbamazepine in the previous therapy (OR = 3.25, CI 1.02–10.32, р = 0.039).
The basis for a long-term rTMS efficacy is normal values of metabolic activity according to PET (OR = 31.49, CI 1.4–71.9, р = 0.025) (fig. 4).
Conclusions
The QOL assessment in epilepsy is necessary for monito–ring patients’ states and estimating the efficacy of a corrective therapy.
The questionnaire QOLIE‑31 is a reliable and sensitive tool of QOL assessment which lets control various components of vital activity.
The results obtained indicate a significant role of attacks frequency and severity and of emotional affective disorders in the subjective assessment of patients’ well-being. Correcting these states with magnetic stimulation positively influences subjects’ everyday functioning increasing the sensation of satisfaction with their quality of life.
Analyzing the results of the conducted research using rTMS and low doses of AEDs showed that such a combination of pharmaceuticals and physical factors let control an epilepsy course improving thereby the quality of life.
The efficacy of combined therapy using rTMS depends on a number of factors the most favorable of which is the lack of significant structural damages according to diffuse tensor MRI, the attack frequency not more than 3 a week, disease duration less than 10 years. The mentioned predictors let perform rTMS with a reliable result of its efficacy.
Using rTMS in a complex therapy for epilepsy allows to minimize the appearance of side-effects of AEDs and provides a high enough anticonvulsant action.
As a result of our study, we obtained the data letting reasonably add a rTMS course to drug therapy for epilepsy and get not only an optimal therapeutic effect for each patient with a minimal risk of side-effects but improve the quality of his/her life.
Conflicts of interests. Authors declare no conflicts of interests.
Список литературы
1. Власов П.Н. Некоторые практические аспекты терапии эпилепсии у взрослых // Consilium medicum. — 2004. — 6(2). — 116-124.
2. Гехт А.Б. Качество жизни больных эпилепсией. Международная конференция «Эпилепсия — диагностика, лечение, социальные аспекты». — М., 2005. — 120-125.
3. Громов С.А., Михайлов В.М., Вассерман Л.И., Лынник С.Д., Флерова И.Л. Качество жизни и реабилитация больных эпилепсией // Журн. неврол. и психиатр. — 2002. — 4-8.
4. Кабанов М.М., Бурковский Г.В. Редукция стигматизации и дискриминации психических больных // Обозрение психиатрии и мед. психологии. — 2000. — 1. — 3-8.
5. Карлов В.А. Эпилепсия у детей и взрослых женщин и мужчин: Руководство для врачей. — Медицина, 2010. — 720 с.
6. Кистень О.В., Евстигнеев В.В., Улащик В.С., Дубовик Б.В. Транскраниальная магнитная стимуляция в диагностике и лечении эпилепсии // Новости медико-биологических наук. — 2009. — 4. — 99-108.
7. Кистень В.В. Транскраниальная магнитная стимуляция в эпилептологии / О.В. Кистень, В.В. Евстигнеев. — Вильнюс: Grafija, 2013. — 368 с.
8. Кистень О.В. Возможные противосудорожные механизмы ритмической транскраниальной магнитной стимуляции и предикторы ее эффективности / О.В. Кистень, В.В. Евстигнеев // Эпилепсия и пароксизмальные состояния. — 2014. — 6/1. — 18-23.
9. Михайлов В.А. Качество жизни, стигматизация и восстановительная терапия больных эпилепсией: Автореф. дис… д-ра мед. наук. — СПб., 2008. — 49 с.
10. Меликян Э.Г., Мильчакова Л.Е., Гехт А.Б. Качество жизни в эпилептологии // Журнал неврол. и психиатр. имени С.С. Корсакова. — 2008. — Вып. 3. Эпилепсия. — 9-11.
11. Незнанов Н.Г., Громов С.А., Михайлов В.А. и др. Эпилепсия, качество жизни, лечение. — СПб.: ВМА, 2005. — 294 с.
12. Пылаева О.А. Воронкова К.В., Петрухин А.С. Побочные эффекты и осложнения антиэпилептической терапии // Фарматека. — 2004. — 9/10. — С. 33-41.
13. Особенности структурных изменений белого вещества мозга в клинической реализации эпилепсии / О.В. Кистень, В.В. Евстигнеев, Р.А. Сакович, И.В. Булаев // Эпилепсия и пароксизмальные состояния. — 2013. — 5/1. — 15-22.
14. Ушкалова Е.А. Влияние антиконвульсантов на качество жизни больных эпилепсией // Фарматека. — 2003. — 16. — 29-40.
15. Юцкова Е.В., Авакян Г.Н., Татаринова М.Ю. Качество жизни и фармакоэкономические особенности лечения эпилепсии у женщин // Журнал неврол. и психиатр. им. С.С. Корсакова. — 2007. — 107(1). — 52-55.
16. Baker G.A. Assessment of quality of life in people with epilepsy: some practical implications // Epilepsia. — 2001. — 42(3). — 66-69.
17. Berto P. Quality of life in patients with epilepsy and impact of treatments // Pharmacoeconomics. — 2002. — 20. — 1039-1059.
18. Cramer J.A., Perrine K., Devinsky O. et al. Development and cross-cultural translation of a 31-item quality of life questionnaire (QOLIE‑31) // Epilepsia. — 1998. — 39. — 81-88.
19. Cramer J.A., Blum D., Reed M. Epilepsy Impact Project Group. The influence of comorbid depression on quality of life for people with epilepsy // Epilepsy Behav. — 2003. — 4. — 15-21.
20. Definition of drug resistant epilepsy: Consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies / P. Kwan, A. Arzimanoglou, A.T. Berg [et al.] // Epilepsia. — 2010. — Vol. 51, № 6. — Р. 1069-1077.
21. Evstigneev V.V. The effect of structural white matter abnormalities on the clinical course of epilepsy / V.V. Evstigneev, V.V. Kistsen, I.V. Bulaev, R.A. Sakovich // Adv. Clin. Exp. Med. — 2013. — Vol. 22, № 4. — 529-537.
22. Hauser W.A. Recent developments in epidemiology of epilepsy // Acta Neurolog. Scandinavica. — 1995. — 162. — 17-21.
23. Kendrick A. Quality of life. The clinical psychologist’s handbook of epilepsy: assesment and management / Ed. by C. Cull, Goldstein. — London; New York, 1997. — 171-176.
24. Kirby S., Sadler R.M. Injury and death as a result of seizures // Epilepsia. — 1995. — 36. — 25-28.
25. Repetitive transcranial magnetic stimulation effects in picrotoxin mo–del of convulsions / V.V. Evstigneev, V.V. Kistsen, B.V. Dubovic, V.S. Ulashchic // Adv. Clin. Exp. Med. — 2016. — Vol. 25, № 2. — P. 317-325.
26. Saillet S., Langlois M., Feddersen B., Minotti L. et al. Manipulating the epileptic brain using stimulation: a review of experimental and clinical studies // Epileptic Disord. — 2009. — 11(2). — 100-112.

/13-19/16-2.jpg)
/13-19/17-1.jpg)
/13-19/18-1.jpg)